
.webp)
In this article
Cortisol gets blamed for a lot these days. Scroll through social media, and you might think it's the root cause of every symptom a woman over 40 experiences. The reality is more nuanced—and far more interesting. Cortisol isn't a villain. It's your body's primary stress-response hormone, and in short bursts it's genuinely protective: it sharpens alertness, raises blood sugar when you need fuel fast, and helps your body mount a "fight-or-flight" response when real threats arise.
The trouble starts when stress is chronic, your sleep is poor, and your cortisol signal stays turned on far longer than your body was designed to handle. In that context, elevated cortisol levels can worsen your fatigue, promote weight gain, trigger insomnia, and aggravate the brain fog that already define hypothyroidism and menopause. Understanding why—and what to do about it—is the focus of this article.
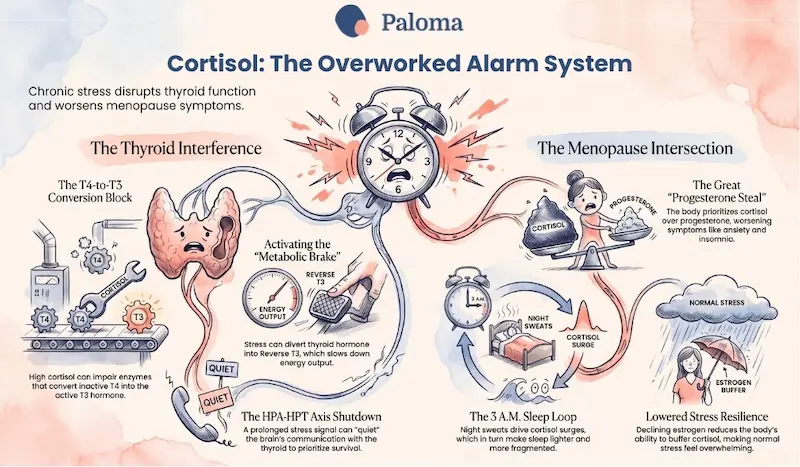
"Cortisol is less of a villain, and more an overworked alarm system that refuses to shut off."
Cortisol is produced by the adrenal glands, the small hormone-secreting structures that sit atop each of your kidneys. It follows a natural daily rhythm: cortisol levels peak shortly after waking to give you energy for the day, then gradually decline, reaching their lowest point in the evening to allow for sleep. This cortisol awakening response is one of the reasons why, under healthy conditions, you feel alert in the morning and wind down at night.
When stress is chronic—whether from work pressure, caregiving demands, poor sleep, or ongoing illness—this natural rhythm can become inverted or flattened. Morning cortisol levels may be blunted (leaving you dragging), while evening cortisol stays high (leaving you lying awake). That "tired but wired" feeling, where you're exhausted but can't switch off, is a hallmark of cortisol dysregulation. And it sets the stage for a cascade of downstream effects on everything from your metabolism to your immune system.
The thyroid and the stress system are deeply connected through the brain's hormone feedback loops—a network sometimes called the HPA axis (hypothalamic-pituitary-adrenal) and HPT axis (hypothalamic-pituitary-thyroid). Because the hypothalamus coordinates both, a prolonged, high-priority stress signal can effectively quiet the thyroid signal to prioritize your survival.
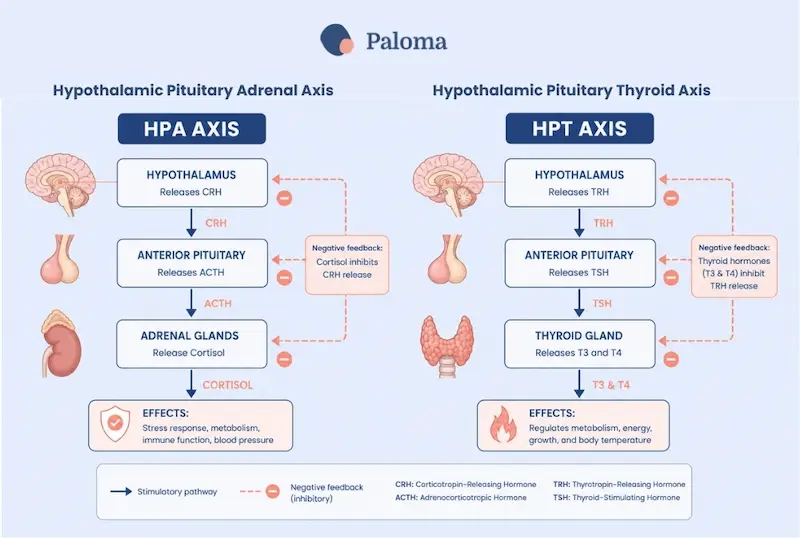
The T4-to-T3 conversion problem
Your thyroid produces mostly T4, an inactive storage form of thyroid hormone. To actually fuel your cells, T4 must be converted into T3, the biologically active thyroid hormone. Research shows that sustained cortisol elevation can suppress the release of TRH and thyroid-stimulating hormone (TSH) from the hypothalamus, disrupt TSH's normal daily rhythm, and—critically—impair the enzymes that convert T4 into T3. The result: even if your labs look 'normal' on a standard TSH test, your tissues may be starved of active thyroid hormone.
High cortisol levels can also divert T4 conversion toward Reverse T3 rather than active T3. Think of rT3 as a metabolic brake: it occupies the same cellular receptors that T3 uses but produces no metabolic effect, effectively slowing down your body's energy output. Studies in hypothyroid patients have found associations between cortisol levels and thyroid markers, lending biological credibility to what many patients have long suspected: feeling hypothyroid despite 'normal' labs may sometimes involve a stress-cortisol component.
The Hashimoto's connection
For people with Hashimoto's disease or other autoimmune thyroid conditions, the cortisol story adds another layer. Chronic stress may heighten inflammatory and immune pressure, potentially making symptoms of hormonal imbalance feel more intense or recovery feel slower. Stress doesn't cause Hashimoto's, but it may significantly influence how much the condition disrupts daily life—and whether a standard medication dose still feels adequate.
A common scenario: a woman with Hashimoto's finds that her usual dose of thyroid medication feels less effective during a period of caregiving stress, fragmented sleep, and skipped meals. Her thyroid labs may still look fine. But the cortisol load is worsening fatigue and brain fog through a parallel pathway. In practice, both the thyroid disorder and the stress response may need attention at the same time.
Perimenopause—the transitional years before menopause—can last up to ten years, and it's rarely a smooth ride. As estrogen and progesterone begin to fluctuate, sleep becomes harder, temperature regulation fluctuates, your mood can shift, and stress tolerance often drops. Some researchers and clinicians suggest that declining estrogen and progesterone may reduce the body's ability to buffer cortisol surges, so that stress that once felt manageable now feels overwhelming.
The symptom overlap between perimenopause and cortisol dysregulation is so significant that it can be genuinely difficult to tell them apart. Both can produce insomnia, irritability, weight gain around the middle, anxiety, low energy, low libido, and brain fog. The honest clinical answer is often: it's both. The menopausal transition lowers resilience, and chronic stress makes the transition feel considerably rougher than it might otherwise be.
The progesterone steal
Progesterone and cortisol share a common precursor called pregnenolone. When the body faces a perceived threat, it prioritizes cortisol production—in effect, "stealing" raw materials that would otherwise be used to make progesterone. This pregnenolone steal can exacerbate classic perimenopausal symptoms like anxiety, insomnia, and irregular cycles, because progesterone plays a crucial calming, sleep-supporting role. When stress consumes the supply, that calming effect diminishes.
The sleep-cortisol loop
One of the most clinically important dynamics in perimenopause is the sleep-cortisol feedback loop. Night sweats, waking at 3 a.m., and difficulty returning to sleep all drive cortisol dysregulation. Elevated stress hormones, in turn, make sleep lighter and more fragmented. Many midlife women find themselves caught in this cycle, where poor sleep worsens hormonal symptoms. This disruption in circadian rhythm can also interfere with sleep. Breaking the loop—often starting with sleep—can be one of the most powerful interventions available.
By the time menopause is established (defined as 12 consecutive months without a period), estrogen is substantially lower, and progesterone is typically very low. Many women notice more pronounced sleep disruption, mood changes, joint discomfort, and shifts in body composition. Stress can amplify menopause symptoms by adding another physiological burden to a system already in transition.
Hot flashes and night sweats are driven primarily by menopause biology—specifically by the narrowing of the thermoregulatory zone in the brain as estrogen declines. But cortisol can worsen the experience and hormonal imbalance by increasing overall arousal, reducing sleep's restorative effects, and potentially contributing to abdominal fat accumulation. This is partly why many women describe a turning point in midlife: 'I used to handle stress fine. Now everything shows up in my body.'
Hot flashes are driven by the biology of menopause. But cortisol can worsen the experience—by increasing arousal, disrupting sleep, and contributing to abdominal weight gain.
It's worth being clear here: the best-supported treatment for bothersome vasomotor symptoms in appropriate candidates remains hormone therapy, not adrenal supplements or cortisol tests purchased from social media ads. The 2022 position statement from The Menopause Society (formerly NAMS) emphasizes hormone therapy as the most effective treatment for vasomotor symptoms and genitourinary syndrome of menopause in eligible patients. Cortisol-focused marketing can distract from treatments that actually work—which is why it's worth separating signal from noise.
No single symptom confirms that cortisol is the issue, and many of the symptoms associated with cortisol dysregulation also overlap with hypothyroidism, depression, sleep apnea, anemia, and other conditions. That said, certain patterns are worth noting:
- Trouble falling asleep, or waking between 2 and 4 a.m., and lying awake for hours
- Feeling tired but also keyed up, wired, irritable, or anxious
- Stronger cravings, especially for sugar or salty foods, particularly in the afternoon or evening
- Weight gain around the midsection that doesn't respond well to diet or exercise
- Worsening brain fog, low motivation, or feeling emotionally depleted
- Symptom flares that coincide with stressful periods or several nights of poor or “short” (less than 7 hours) sleep
If these patterns sound familiar, it's worth bringing them up with your clinician—not to diagnose yourself with “adrenal fatigue,” but to ensure that the stress dimension of your symptom picture is being considered alongside your thyroid and hormone workup.
Standard thyroid panels often only include TSH. If you suspect cortisol-thyroid interactions, a more comprehensive workup might include Free T3, Free T4, Reverse T3, and thyroid peroxidase antibodies (TPOAb). These give a fuller picture of how well thyroid hormone is being produced, converted, and used.
For cortisol specifically, a single blood draw is limited because cortisol fluctuates throughout the day. A salivary cortisol test taken at four time points—waking, mid-morning, afternoon, and evening—maps your daily cortisol curve and can reveal whether levels are high at night, blunted in the morning, or otherwise dysregulated. This kind of functional testing is most useful when interpreted by a clinician familiar with the full hormonal picture, rather than ordered from a direct-to-consumer lab without guidance.
True cortisol disorders—Cushing syndrome (excess cortisol) and Addison’s disease (inadequate cortisol production)—are relatively rare but clinically serious. If your clinician suspects either, a formal medical evaluation with appropriate lab protocols is essential. These conditions are distinct from the lifestyle-driven cortisol dysregulation described in this article and require entirely different treatment.
Treatment should be guided by the underlying problem, not the hormone label. If hypothyroidism is the primary issue, the first step is to confirm that thyroid hormone replacement therapy is appropriate and optimized for you, since uncontrolled thyroid disease can mimic stress-related symptoms in both directions. Some evidence suggests that addressing chronic stress may support thyroid regulation, but it is not a substitute for thyroid medication when one is needed.
If menopausal symptoms are the main concern, evidence-based treatment includes menopausal hormone therapy for appropriate candidates, or nonhormonal alternatives. These options include certain antidepressants, gabapentin, or the recently approved neurokinin receptor antagonist fezolinetant (Veozah) when hormone therapy isn't a fit. For sleep disruption, anxiety, or mood changes that persist despite hormone management, cognitive behavioral therapy for insomnia (CBT-I) has strong evidence, but it’s often underutilized as a first-line option.
Lifestyle changes don't replace needed medical care, but they can meaningfully reduce how much cortisol dysregulation compounds your symptoms day to day. The following are among the most evidence-supported approaches:
Prioritize sleep above almost everything else
Sleep is the primary window for endocrine repair. When you're sleep-deprived, cortisol levels are artificially elevated the following day, worsening insulin sensitivity and impairing thyroid hormone conversion. Consistent sleep and wake times—even on weekends—anchor your cortisol rhythm. Morning light exposure within 30 minutes of waking helps reinforce the cortisol awakening response. Keeping screens out of the bedroom and maintaining a cool sleep environment can reduce the frequency of night waking.
Eat to stabilize blood sugar
Skipping meals, undereating, or relying heavily on caffeine and simple carbohydrates can drive blood sugar swings that act as physiological stressors. Balanced meals anchored by protein, fiber, and healthy fats—eaten at consistent times—reduce the glucose spikes and crashes that trigger cortisol responses. Limiting alcohol and caffeine, particularly after noon, can also help preserve sleep quality.
Choose movement that restores rather than depletes
High-intensity exercise is a stressor—meaning small doses are beneficial, but large or frequent doses can backfire when your system is already depleted. Resistance training and consistent moderate movement preserve muscle mass, support insulin sensitivity, and improve cortisol metabolism without triggering the large adrenal demand that intensive cardio can. Walking, swimming, yoga, and strength training are generally well tolerated, even during periods of high stress.

Build brief, consistent stress-recovery practices
Stress management works best when it's practical and consistent rather than occasional and effortful. Even five minutes of slow, diaphragmatic breathing before bed can shift the nervous system away from high-alert mode. Journaling, meditation, brief walks in nature, and deliberate downtime between tasks can all reduce the cumulative cortisol burden throughout the day.
Navigating the intersection of cortisol, thyroid, and menopause is complex, and the most useful conversations happen when you come prepared. Here are some questions worth raising:
- "My symptoms feel out of proportion to my labs—could stress or sleep be playing a role?"
- "Would testing Free T3, Reverse T3, or thyroid antibodies give a more complete picture?"
- "Which of my symptoms are most likely hormonal, and which might need a sleep or mental health evaluation?"
- "Am I a candidate for hormone therapy, or if not, what nonhormonal options are best supported by evidence?"
- "Would a diurnal cortisol test be useful in my case?"
Cortisol may not be the entire explanation for why thyroid and menopause symptoms feel harder than expected—but it can be a meaningful and underappreciated piece of the puzzle. Once that piece is identified and addressed alongside proper medical management of the underlying conditions, the full picture often becomes clearer, and treatment becomes considerably more targeted and effective.
You are not failing at wellness. You are navigating a genuinely complex physiological transition, and your body's signals deserve a thorough investigation—not just a reassurance that your labs are "normal."
If stress, hypothyroidism, and menopause symptoms seem to be piling on all at once, you don't have to figure it out alone. At Paloma, our thyroid specialists understand that fatigue, brain fog, weight changes, poor sleep, and mood shifts often have multiple overlapping causes. That's why we look beyond a single lab value, using comprehensive and convenient thyroid testing, personalized treatment plans, medication management, and ongoing support to help you optimize your thyroid health.
By optimizing your thyroid function and addressing lifestyle factors like stress, sleep, and nutrition, you can feel more like yourself again. If you're ready for expert thyroid care that's designed around you, Paloma is here to help you take the next step toward better health.
understand the connection
Perimenopause, Menopause, and Hypothyroidism
Gain insights into how these conditions are linked and how to manage your health effectively.

Can high cortisol make hypothyroidism symptoms worse?
Yes. Chronic elevations in cortisol can interfere with thyroid hormone signaling and the conversion of T4 to active T3, potentially worsening fatigue, brain fog, and weight gain even when your thyroid lab results appear normal.
Can stress actually cause hypothyroidism?
Stress alone doesn't cause hypothyroidism or Hashimoto's disease. However, chronic stress can worsen symptoms, increase inflammation, and make an existing thyroid condition more difficult to manage.
Why do menopause and high cortisol feel so similar?
Both menopause and cortisol dysregulation can cause insomnia, anxiety, mood swings, weight gain, and difficulty concentrating. Because the symptoms overlap so closely, many women are actually experiencing a combination of both hormonal changes and chronic stress.
Can cortisol affect thyroid medication?
Indirectly, yes. Elevated cortisol may reduce the body's ability to efficiently use thyroid hormone by impairing T4-to-T3 conversion, which can leave some people feeling hypothyroid despite taking their prescribed medication.
Is waking up at 3 a.m. a sign of high cortisol?
Frequent early-morning awakenings can be a sign of cortisol dysregulation, especially if you're exhausted but unable to fall back asleep. However, thyroid disease, menopause, sleep apnea, and other medical conditions can also cause nighttime waking.
Should I get my cortisol levels tested?
Testing may be appropriate if your symptoms suggest a cortisol imbalance, but it should be guided by your healthcare provider. When needed, a multi-point salivary cortisol test often provides more useful information than a single blood test.
What is the connection between cortisol and weight gain?
Chronically elevated cortisol can increase appetite, encourage cravings for sugary foods, and promote fat storage around the abdomen. Combined with hypothyroidism or menopause, these effects can make losing weight considerably more challenging.
Can lowering stress improve thyroid health?
Managing stress won't cure hypothyroidism, but it may reduce the burden that chronic cortisol places on your body. Better sleep, regular movement, and effective stress management can complement appropriate thyroid treatment and help improve overall well-being.
Are supplements enough to fix cortisol problems?
Usually not. While some supplements are heavily marketed for "adrenal support," the strongest scientific evidence supports addressing sleep, nutrition, exercise, stress, and any underlying thyroid or menopausal conditions with appropriate medical care.
How can I tell if my symptoms are from cortisol, menopause, or my thyroid?
It isn't always possible to separate them based on symptoms alone because they overlap so extensively. A comprehensive evaluation—including thyroid testing, a review of menopausal symptoms, sleep patterns, stress levels, and overall health—can help determine which factors are contributing most to how you feel.
.webp)



.webp)
%20(1).webp)





