
.webp)
In this article
Feeling chronically fatigued, experiencing brain fog, or struggling with unexplained weight gain, yet your doctor tells you that your thyroid tests are “perfectly normal?” This is a common and deeply frustrating experience for many people.
You’ve been to the doctor. You know something isn’t right; your body is sending distress signals. You’ve had the blood work done. And there it is in black and white: your thyroid-stimulating hormone (TSH) is “normal.” It’s “in range.” By every standard lab measure, your thyroid is functioning normally. Your doctor smiles and says, “Everything looks good.”
But you’re exhausted. Not that tired-after-a-long-week feeling, but a bone-deep, alarm-ignoring, can’t-push-through total exhaustion and worsening chronic fatigue. You’ve gained weight you can’t explain. You’re cold when everyone else is comfortable. You’re down, foggy, achy, and increasingly frustrated.
You know your own body, and something is clearly wrong! Yet standard diagnostic tools don’t seem to reflect your lived reality.
If this sounds familiar, you are far from alone — and you are not imagining it.
In Paloma’s community and across social media, this exact experience is one of the most-searched, most-shared, and most emotionally raw conversations happening right now. Post after post describes the same cycle: debilitating symptoms, a doctor’s appointment, bloodwork, and the dreaded “Your levels are normal” dismissal that sends patients home with no answers and no treatment. Patients often feel unheard, dismissed, and unsure of where to turn. Subreddits dedicated to thyroid disease are flooded with threads that begin with some version of: “My TSH is normal, but I feel awful — does anyone else experience this?”
The answer, it turns out, is yes.
And a major 2025 review published in Frontiers in Endocrinology is finally starting to explain why — in terms the medical community can no longer ignore.
Our goal in this article is to demystify euthyroid Hashimoto’s. We’ll explore why symptoms can manifest even when standard thyroid tests show normal TSH levels. We’ll also delve into the limitations of conventional thyroid testing, discuss more comprehensive diagnostic approaches, and highlight the importance of considering other factors such as nutrition, adrenal health, and gut function. Finally, we’ll provide guidance on advocating for yourself within the healthcare system and explore lifestyle strategies to support your thyroid health and alleviate your symptoms, empowering you to take a more proactive role in your well-being.
Hashimoto’s thyroiditis, also known as Hashimoto’s disease or chronic lymphocytic thyroiditis, is the most common cause of hypothyroidism in many developed countries. It is fundamentally an autoimmune condition. This means the body’s immune system, which is designed to protect against foreign invaders such as bacteria and viruses, mistakenly identifies the thyroid gland as a threat.
Understanding the autoimmune attack on your thyroid gland
In Hashimoto’s, the immune system produces antibodies that target and attack the thyroid gland. The most common antibodies involved are thyroid peroxidase (TPO) and thyroglobulin (Tg) antibodies. These antibodies can cause inflammation and damage to the thyroid tissue over time. The thyroid gland itself is a small, butterfly-shaped endocrine gland located at the base of your neck. It plays a crucial role in regulating metabolism by producing thyroid hormones, primarily thyroxine (T4) and triiodothyronine (T3). These hormones influence nearly every cell in your body, affecting energy production, heart rate, body temperature, and numerous other vital functions. The global prevalence of Hashimoto’s thyroiditis is estimated to be between 5 to 10% of the general population, highlighting its significant impact on public health.
The progression of Hashimoto’s: From autoimmunity to hypothyroidism
Hashimoto’s thyroiditis is a progressive disease. The autoimmune attack can lead to gradual destruction of thyroid tissue, impairing the gland’s ability to produce sufficient thyroid hormones. This eventual decline in hormone production results in hypothyroidism, a condition where the thyroid gland is underactive. However, the transition from an active autoimmune state to overt hypothyroidism is not always immediate or linear. Hashimoto’s thyroiditis is the cause of hypothyroidism in more than 70% of patients diagnosed with the condition.
Why the autoimmune process can begin long before overt dysfunction
The immune system’s attack in Hashimoto’s can persist for years, causing ongoing inflammation and damage, even while the thyroid gland is still able to compensate and produce adequate amounts of thyroid hormones. During this compensatory phase, standard blood tests, particularly TSH levels, may remain within the “normal” range. The pituitary gland secretes TSH, which signals the thyroid to produce more hormones. When thyroid hormone levels start to drop, TSH levels rise to stimulate more production. However, before this drop becomes significant enough to elevate TSH above the reference range, the underlying autoimmune process can still be actively causing symptoms. A recent study found that Hashimoto’s patients with normal thyroid levels still experience significant symptoms, including fatigue, brain fog, digestive issues, cold intolerance, and joint pain, with severity often linked to antibody levels. This highlights that the presence of antibodies and ongoing inflammation, rather than just hormone levels, can be the source of symptoms. Furthermore, it takes an average of 4.5 years to diagnose an autoimmune disease, underscoring the potential for prolonged symptom duration before a definitive diagnosis is reached.
The word “euthyroid” simply means that thyroid hormone levels are within the normal reference range. So euthyroid Hashimoto’s describes a state in which a person has been diagnosed with Hashimoto’s — confirmed by elevated thyroid antibodies (typically TPO antibodies and/or thyroglobulin antibodies) and often by ultrasound — but their TSH and free T4 levels both fall within the reference range, at levels labs consider normal.
In conventional medicine, a normal TSH has traditionally been the finish line. If the number is in range, the thyroid is considered “under control,” and symptoms are attributed to other causes: stress, depression, anxiety, aging, and lifestyle. This is where many patients hit a wall.
But research is drawing a much more nuanced picture. Hashimoto’s is not simply a thyroid condition — it is a systemic autoimmune disease. And the thyroid numbers tell only part of the story.
“Your TSH is normal” doesn’t mean the autoimmune process has quieted down. For many patients, the immune system is still very much at war.
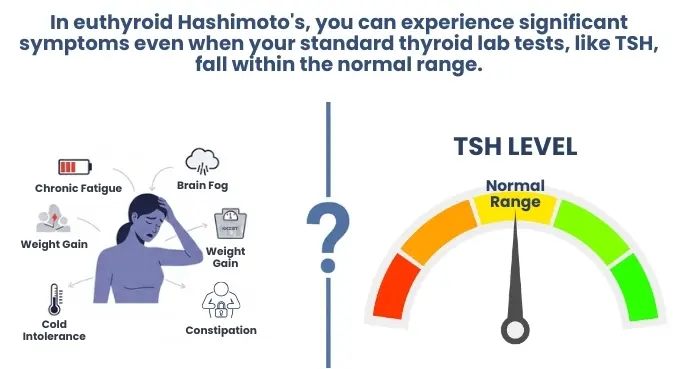
Individuals experiencing euthyroid Hashimoto’s often report a constellation of symptoms commonly associated with hypothyroidism, even though their thyroid hormone levels may appear within the normal range. These symptoms can be wide-ranging and significantly impact daily life:
- Fatigue and low energy: A profound sense of tiredness that is not relieved by rest.
- Brain fog and cognitive impairment: Difficulty concentrating, memory problems, and a feeling of mental sluggishness.
- Weight gain and difficulty losing weight: Metabolic changes can make it harder to maintain a healthy weight.
- Mood disturbances: Increased risk of depression, anxiety, and irritability.
- Temperature intolerance: Feeling excessively cold or, sometimes, unusually warm.
- Digestive issues: Constipation, bloating, or other changes in bowel habits.
- Skin and hair changes: Dry skin, brittle nails, and hair thinning or loss.
- Muscle and joint pain: Aches and stiffness in the body.
- Menstrual irregularities: Changes in menstrual cycles for women.
- Increased cholesterol levels: Even without overt hypothyroidism.
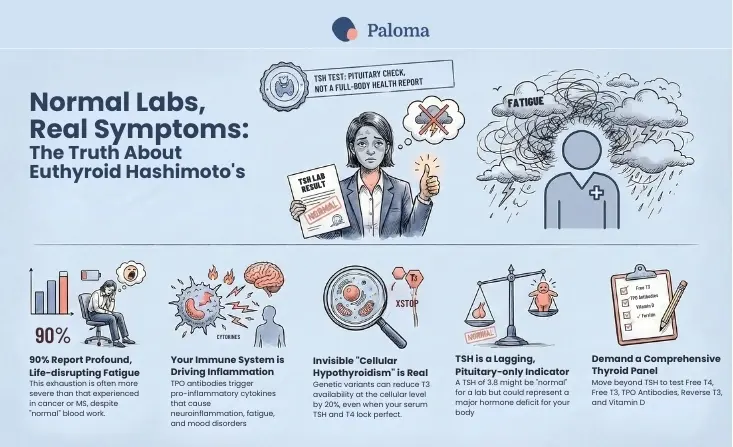
Nearly 90% of people with hypothyroidism report abnormal fatigue — with severity often worse than that experienced by patients with cancer, anemia, multiple sclerosis, and those on kidney dialysis.
According to the 2025 review in Frontiers in Endocrinology, approximately 5 to 10% of patients with Hashimoto’s thyroiditis continue to experience persistent symptoms despite achieving biochemical euthyroidism — meaning normal TSH and free T4. [1] The symptoms these patients describe are strikingly consistent: fatigue, weight gain, cold intolerance, constipation, and depression—the same cluster, again and again, in people whose labs look perfectly fine.
That figure — 5 to 10 percent — may sound modest, but given how prevalent Hashimoto’s is, it translates to a very large number of people being told they are well when they are not. Many researchers believe the true proportion is higher, as persistent symptoms in euthyroid patients are frequently misattributed and never properly counted.
In euthyroid Hashimoto’s, your body feels out of sync, yet the objective data, as interpreted by standard medical protocols, suggests otherwise. This can be particularly perplexing because symptoms like profound fatigue are incredibly debilitating. In fact, nearly 90% of people with hypothyroidism, including those with Hashimoto’s, report abnormal fatigue, with its severity often being worse than that experienced by patients with cancer, anemia, inflammatory bowel disease, multiple sclerosis, and those on kidney dialysis. This statistic underscores how significantly fatigue can impact an individual’s life, even when thyroid hormone levels may appear within normal limits.
Many individuals with euthyroid Hashimoto’s thyroiditis also show lower scores on quality of life scales, particularly in physical and mental health sub-dimensions, compared to matched controls, indicating that effective control of hypothyroidism is not always sufficient to mitigate these negative effects.
The journey to understanding persistent, unexplained symptoms can be arduous. When you present with complaints like fatigue, changes in mood, temperature sensitivity, digestive issues, or cognitive difficulties, and standard blood tests—particularly your thyroid-stimulating hormone (TSH) levels—fall within the laboratory’s reference range, it’s easy to feel invalidated. You are experiencing genuine symptoms, yet the typical markers used to diagnose thyroid dysfunction appear normal. This situation can lead to prolonged periods of uncertainty, repeated doctor visits, and a growing sense of helplessness.
The 2025 study identified several distinct mechanisms that may explain why a Hashimoto’s patient can have a perfectly normal TSH and yet still feel unwell. Understanding these mechanisms is the key to understanding why the standard “your labs are fine” response is, for many patients, simply the wrong answer.
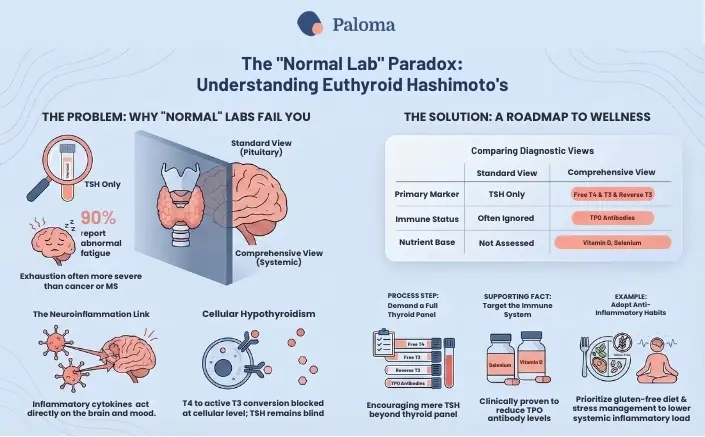
The limitations of the TSH test
TSH — thyroid-stimulating hormone — is produced by the pituitary gland and signals the thyroid to produce more thyroid hormone. When thyroid hormone levels are low, TSH rises to stimulate the thyroid. When levels are high, TSH falls. When doctors check a TSH level, they are mostly checking whether your pituitary gland is functioning properly. But the pituitary’s assessment of thyroid hormone availability may not accurately represent what is actually happening in peripheral tissues throughout the rest of your body. TSH is a lagging indicator.
The HPT (hypothalamic-pituitary-thyroid) axis operates within a tightly regulated but highly individual feedback loop. Research cited in the review shows there is substantial inter-individual variability in TSH set-points, shaped by genetic, metabolic, and environmental factors. [1] What this means in practice: a TSH of 3.8 might be perfectly normal for one person and represent a relative thyroid hormone deficit for another. A population-based reference range cannot account for the fact that your body has its own internal normal, which may differ from the lab’s.
The need for a complete thyroid panel
To gain a more comprehensive understanding, a full thyroid panel is essential. This panel typically includes:
- TSH: To assess the pituitary-thyroid axis.
- Free T4 (FT4): The unbound, active form of thyroxine, readily available for conversion to T3.
- Free T3 (FT3): The most active thyroid hormone, directly influencing cellular metabolism. Many individuals experience symptoms when their FT3 levels are low, even if FT4 and TSH are normal.
- Reverse T3 (rT3): An inactive form of T3 that can increase during times of stress or inflammation, potentially blocking the action of active T3. Elevated rT3 can contribute to hypothyroid-like symptoms.
For individuals suspected of having Hashimoto’s, testing for thyroid antibodies is critical.
- Thyroid Peroxidase Antibodies (TPOAb): Elevated TPOAb levels are highly indicative of Hashimoto’s thyroiditis.
- Thyroglobulin Antibodies (TgAb): Elevated TgAb levels can also be present and are another marker of autoimmune thyroid disease.
The presence of these antibodies confirms an autoimmune attack on the thyroid, even if TSH, FT4, and FT3 levels are currently within the normal range. The severity of symptoms in euthyroid Hashimoto’s patients has been linked to antibody levels, reinforcing the importance of this testing.
The T3 problem: Your body may not be converting properly
Even when TSH looks fine, the active thyroid hormone — T3 (triiodothyronine) — may not be getting where it needs to go. The body converts T4 (thyroxine) to T3 via enzymes called deiodinases, and this conversion can be significantly impaired in some people.
The review highlights a specific genetic variant in the DIO2 gene (a polymorphism) that reduces deiodinase type 2 activity by approximately 20% and is found in 12–36% of the general population. Individuals carrying this variant may have reduced T3 availability at the cellular level even when their serum TSH and T4 are entirely normal — a state researchers describe as tissue-specific hypothyroidism that standard thyroid function tests cannot detect.
This is cellular hypothyroidism in a person with normal labs. It is a real physiological phenomenon, and it is invisible to the test your doctor is ordering.
The autoimmune inflammation driver
This is where the most compelling — and most actionable — science lies. The review synthesizes evidence showing that the autoimmune nature of Hashimoto’s may itself be a direct cause of persistent symptoms, entirely independent of thyroid hormone levels.
A large systematic review from 2021 provides particularly strong evidence: individuals with positive TPO antibodies report significantly higher rates of fatigue, cognitive dysfunction, irritability, and depressive mood, even when TSH and free T4 are completely normal. Of the 30 studies included in that systematic review, the majority found a significant association between thyroid autoimmunity and persistent symptoms or reduced quality of life. The antibodies themselves, and the immune activation they represent, appear to be driving symptoms through a separate pathway.
The mechanism involves pro-inflammatory cytokines. TPO antibody positivity is associated with elevated levels of interleukin-6 (IL-6) and tumour necrosis factor-alpha (TNF-α). These are powerful immune signaling molecules that, when chronically elevated, exert systemic effects extending far beyond the thyroid gland. Critically, IL-6 and TNF-α can influence central nervous system function through neuroinflammatory pathways — and have been directly implicated in the pathophysiology of fatigue, mood disturbances, and altered pain perception.
In other words, your immune system is producing inflammatory signals that are acting on your brain. Your TSH has nothing to do with it.
In addition to thyroid lab tests, it’s also important to evaluate several micronutrients that play vital roles in thyroid hormone production, conversion, and immune function. Deficiencies in these nutrients are common in individuals with autoimmune thyroid disease and can contribute to symptoms:
- Selenium: Essential for the conversion of T4 to T3 and has antioxidant properties that can help protect the thyroid from oxidative stress.
- Zinc: Also involved in thyroid hormone metabolism and immune function.
- Vitamin D: Plays a significant role in immune regulation and is often low in individuals with autoimmune diseases.
- Iron (specifically ferritin): Iron deficiency anemia can mimic or worsen thyroid symptoms and impair thyroid hormone production.
- B Vitamins (especially B12): Crucial for energy production and neurological function, and deficiencies can contribute to fatigue and brain fog.
Understanding these three mechanisms helps explain why the symptom picture in euthyroid Hashimoto’s can be so wide-ranging and yet so consistent across patients. These are not vague or psychosomatic complaints. They are specific, reproducible, and increasingly well-documented.
Fatigue
Fatigue is the symptom patients describe most urgently — not tiredness, but a profound exhaustion that disrupts work, relationships, and daily function. When inflammatory cytokines like IL-6 act on the central nervous system, they suppress neurotransmitter production and disrupt cellular energy metabolism at a fundamental level.
Weight gain and difficulty losing weight
Weight gain and difficulty losing weight are common even in euthyroid patients whose metabolic panels look normal. Chronic systemic inflammation is increasingly recognized as contributing to metabolic dysfunction and altered fat storage, independent of thyroid hormone levels. Reduced T3 at the cellular level further suppresses metabolic rate in ways a TSH test will not reveal.
Cold intolerance
Cold intolerance — feeling perpetually chilled, especially in the extremities — is often reflexively attributed to low thyroid hormone levels. But in euthyroid patients, impaired peripheral T3 availability and inflammatory changes in circulation can produce the same symptom.
Depression and anxiety
Depression and anxiety may be the most underrecognized symptoms in this population. Given the established link between elevated TNF-α, IL-6, and mood disorders, and the dramatically elevated odds ratios for depression and anxiety in Hashimoto’s patients documented in the Siegmann et al. meta-analysis [3], these symptoms have a plausible neuroinflammatory explanation — not a purely psychological one.
Brain fog
Brain fog — difficulty concentrating, memory lapses, word-finding struggles, slowed thinking — is nearly universal in patient-reported accounts. Cognitive dysfunction and irritability are specifically named in the Groenewegen systematic review [2] as symptoms associated with TPO antibody positivity independent of thyroid hormone status.
A normal TSH doesn’t mean a Hashimoto’s patient is well. It means their pituitary gland is satisfied. Those are not the same thing.
There is no single universal treatment protocol, and this remains an area of active research. There is currently no consensus on how to manage persistent symptoms in euthyroid Hashimoto’s patients. But there is growing evidence for several targeted strategies. The key is working with a clinician who looks beyond the TSH.
Selenium supplementation
Selenium is among the best-studied interventions in the management of Hashimoto’s. The thyroid gland has the highest selenium concentration of any organ in the body; selenium-dependent enzymes are essential for antioxidant defense and thyroid hormone metabolism.
A 2016 meta-analysis found that selenium supplementation significantly reduced TPO antibody levels in LT4-treated patients at 3, 6, and 12 months. A more recent and comprehensive meta-analysis from 2024 confirmed these findings across 2,358 participants, showing significant reductions in TPO antibodies regardless of whether patients were on thyroid hormone replacement therapy.
Lower TPO antibody titers are a meaningful target because TPO antibody positivity drives the pro-inflammatory cytokine cascade. Selenium supplementation is particularly recommended in patients with documented selenium deficiency. If you have Hashimoto’s, discussing selenium with your provider is an evidence-informed conversation worth having.
Vitamin D supplementation
Low vitamin D levels are consistently observed in patients with autoimmune thyroiditis, and the review [1] explains a plausible mechanistic reason: vitamin D helps restore immune tolerance by modulating T-cell activity and cytokine profiles. Specifically, research suggests vitamin D can prevent dendritic-cell-dependent T-cell activation, reduce inflammatory cytokine production, and restore the Th17/Treg ratio — an immune balance that is disrupted in Hashimoto’s.
Some studies found that vitamin D supplementation in patients with deficient Hashimoto’s disease led to decreased thyroid autoantibody titers and improved thyroid function. The evidence quality is rated as low-to-moderate, but given the consistent finding of vitamin D deficiency in this population and its established role in immune regulation, testing and correcting vitamin D levels is a reasonable and low-risk step.
Dietary foundations for autoimmune support
An anti-inflammatory diet is fundamental for managing autoimmune conditions. Focusing on whole, unprocessed foods can help calm the immune system and reduce inflammation. Key dietary considerations include:
- Eliminating Inflammatory Triggers: Many individuals with Hashimoto’s find benefit from removing gluten and dairy, as these are common inflammatory foods.
- Nutrient-Dense Foods: Emphasize plenty of fruits, vegetables, lean proteins, and healthy fats.
- Adequate Protein Intake: Protein is essential for hormone production and repair.
- Iodine Considerations: While iodine is necessary for thyroid hormone production, excessive intake can be detrimental for individuals with Hashimoto’s, potentially triggering or worsening the autoimmune response. It is important to discuss iodine intake with a healthcare provider, as supplements or certain diets can provide very high levels.
- Focus on Gut Health: Incorporate fermented foods (like sauerkraut and kimchi) and fiber-rich foods to support a healthy gut microbiome.

Stress management techniques

Chronic stress is a significant contributor to HPA axis dysregulation and can exacerbate autoimmune conditions. Implementing stress management techniques is crucial:
- Mindfulness and Meditation: Regular practice can help calm the nervous system.
- Deep Breathing Exercises: Simple yet effective for immediate stress reduction.
- Yoga or Tai Chi: Gentle forms of movement that combine physical activity with mindfulness.
- Prioritizing Sleep: Aim for 7-9 hours of quality sleep per night, as sleep is critical for hormonal balance and immune system recovery.
Lifestyle strategies to support thyroid health and alleviate symptoms
Beyond diet and stress management, consistent, gentle lifestyle habits can significantly impact well-being:
- Regular, gentle exercise: While intense exercise can sometimes exacerbate inflammation, regular moderate activity like walking, swimming, or yoga can improve energy levels, mood, and circulation.
- Adequate hydration: Drinking sufficient water is essential for all bodily functions, including metabolism and detoxification.
- Consider targeted supplementation: Under the guidance of a healthcare professional, key nutrients like Selenium, Vitamin D, Zinc, and B vitamins may be recommended to address deficiencies and support thyroid function and immune health.
- Limiting exposure to environmental toxins: Reducing exposure to endocrine-disrupting chemicals found in plastics, personal care products, and processed foods can support overall hormonal health.
This may be the most surprising finding in the study. For a carefully selected subset of patients with severe symptoms that have not responded to any other approach, total thyroidectomy is emerging as a legitimate therapeutic consideration.
The logic is compelling: by removing the thyroid gland entirely, you remove the primary antigenic stimulus driving the autoimmune response. Post-operatively, TPO antibody levels fall dramatically, and with them, the inflammatory cytokine activity that appears to underlie many symptoms. The only randomized controlled trial available demonstrated significant improvements in fatigue and quality of life at 6, 12, and 18 months after total thyroidectomy compared to continued medical therapy. The surgery group’s SF-36 general health score increased by 26 points while the control group’s showed no change; rates of chronic fatigue dropped from 82% to 35% in the surgical group. These improvements occurred alongside marked reductions in TPO antibody levels.
A 2024 observational follow-up study supported these findings, confirming the beneficial and lasting effects of total thyroidectomy in euthyroid Hashimoto’s patients with persistent symptoms.
One cost-effectiveness analysis found that total thyroidectomy may be both more effective and less costly over the long term than ongoing medical management in severely symptomatic patients — largely because of the substantial indirect costs of Hashimoto's-associated depression and anxiety (lost productivity, ongoing treatment).
This is not a first-line option and comes with real surgical risks — the review notes elevated rates of transient hypoparathyroidism in HT patients specifically (15.3%) due to dense inflammatory tissue, making parathyroid preservation more difficult. Surgery should be reserved for patients who have exhausted conservative options, and decisions must involve multidisciplinary evaluation and genuine shared decision-making. But it belongs in the conversation for patients who have been suffering for years with no relief.
While the study focused primarily on medical interventions, the picture it paints strongly supports the role of an anti-inflammatory lifestyle . If chronic elevation of cytokines is driving symptoms, then any evidence-based approach that reduces inflammation is relevant.
An anti-inflammatory diet — emphasizing vegetables, fruits, fatty fish, olive oil, nuts, and seeds while reducing processed foods and refined sugar — is consistently associated with lower levels of inflammatory markers in clinical research. For patients with co-occurring gluten sensitivity or celiac disease (which occurs at higher rates in Hashimoto’s patients), a gluten-free approach may provide additional benefit.
Chronic psychological stress powerfully upregulates the same pro-inflammatory pathways implicated in euthyroid Hashimoto’s, making stress management a physiologically grounded priority. Sleep optimization matters equally: disrupted sleep amplifies inflammatory signaling, worsening the very cytokine cascades that may be driving symptoms.
The study also examined traditional Chinese medicine (TCM) approaches, acknowledging growing interest in their potential. A meta-analysis of 16 trials of Chinese herbal formulas found that certain formulations reduced both TPO and thyroglobulin antibody levels. Pharmacological evidence suggests these herbs may work by downregulating pro-inflammatory cytokines — the same targets implicated in euthyroid Hashimoto’s symptoms. A systematic review and meta-analysis of 14 randomized controlled trials also found that acupuncture significantly reduced TPO antibody levels and increased thyroid hormone levels compared with levothyroxine alone.

Effective management of euthyroid Hashimoto’s requires a diagnostic framework that goes far beyond a single TSH value. A comprehensive thyroid panel — including free T3, free T4, and TPO antibodies — gives a far richer picture of immune activity and hormone conversion. Tracking antibody levels over time provides meaningful data about whether interventions are working.
Given the evidence linking deficiencies to both immune dysregulation and symptom burden in Hashimoto’s patients, vitamin D, ferritin, and B12 levels should also be assessed. Inflammatory markers like C-reactive protein (CRP) can provide additional context, especially for patients exploring whether their symptom burden tracks with inflammatory activity.
Understanding euthyroid Hashimoto’s is the first step, but navigating the healthcare system to get the necessary diagnosis and support can be challenging. Your proactive engagement is key.
Effective communication with your healthcare provider
When you have your appointment, be prepared. Clearly articulate your symptoms, their duration, and how they impact your daily life. Bring a list of symptoms, questions, and any previous lab results. Don’t hesitate to explain that you suspect euthyroid Hashimoto’s and request specific tests such as a full thyroid panel (including Free T4, Free T3, Reverse T3) and thyroid antibodies. Use your research to inform your requests and present them respectfully. Remember, your provider is a partner in your health journey, and clear communication can foster a collaborative approach.
Seeking specialized expertise
If your primary care provider is not receptive to further testing or does not have expertise in thyroid disorders, consider seeking out specialists like Paloma Health, with expertise in managing Hashimoto’s and hypothyroidism. Additionally, functional medicine practitioners or naturopathic doctors often have a deeper understanding of autoimmune conditions and the nuances of thyroid dysfunction, focusing on identifying root causes and implementing comprehensive treatment plans.
The value of a second opinion
If you feel your concerns are not being adequately addressed or if you receive a diagnosis that doesn’t align with your understanding, don’t hesitate to seek a second opinion. It is your right to explore different perspectives and ensure you are receiving the most appropriate care for your condition.
Euthyroid Hashimoto’s is not a diagnosis of exclusion. It is not stress. It is not anxiety. And it is not something you should have to fight to have taken seriously. It is a real, increasingly well-characterized phenomenon in which an active autoimmune process drives systemic inflammation — including neuroinflammation — in ways that a TSH number simply cannot capture.
The 2025 Frontiers in Endocrinology review is significant precisely because it synthesizes the full picture: the limitations of TSH, the T3 conversion problem, and the inflammatory pathways linking TPO antibody positivity to fatigue, mood disorders, brain fog, and pain. It validates what patients have been reporting for years. And it provides a clear rationale for moving beyond the TSH-centric model of thyroid care.
If you have Hashimoto’s and you don’t feel well despite normal labs, push for comprehensive testing. Seek out a provider who evaluates antibody levels, inflammatory markers, free T3, and your full symptom picture. Explore the evidence-backed interventions available to you. And know that the science is catching up — your experience has always been real, and now the research is beginning to explain exactly why.
The experience of euthyroid Hashimoto’s—feeling unwell despite normal thyroid tests—is a testament to the complexity of thyroid health and the limitations of conventional diagnostic approaches. Your symptoms are real and valid, and they deserve a thorough investigation. Hashimoto’s thyroiditis, an autoimmune condition, can silently disrupt your thyroid gland’s function and impact your overall well-being long before standard blood tests reflect overt hypothyroidism. By understanding that autoimmune process, recognizing the limitations of TSH as a sole marker, and advocating for comprehensive testing that includes thyroid antibodies and hormone levels (Free T3, Free T4, Reverse T3), you can gain real clarity.
Empowering yourself with knowledge and proactively engaging with a healthcare provider like Paloma is paramount. In addition, embracing lifestyle strategies focused on an anti-inflammatory diet, effective stress management, quality sleep, and targeted supplementation can significantly alleviate symptoms and support your thyroid’s health.
Remember that diagnosing and managing euthyroid Hashimoto’s is a journey, and with persistence, a comprehensive approach, and self-advocacy, you can navigate this path toward better health and reclaim your vitality.
What does “euthyroid Hashimoto’s” actually mean?
“Euthyroid” simply means your thyroid hormone levels are within the normal reference range — so euthyroid Hashimoto’s describes the condition where you’ve been diagnosed with Hashimoto’s (confirmed by elevated antibodies and/or ultrasound). Yet, your TSH and T4 come back within the reference range. It’s the medical term for the incredibly common experience of “my labs are normal, but I feel terrible.”
If my TSH is normal, why do I still feel so awful?
Because TSH only tells you what your pituitary gland thinks — it does not tell you what’s happening in the rest of your body. In Hashimoto’s, your immune system produces inflammatory molecules called cytokines that act directly on your brain and nervous system, driving fatigue, mood changes, and brain fog, independent of your thyroid hormone levels. Your labs can be “normal,” and your immune system can still be very much at war.
How common is this? Am I really not alone?
Extremely common. Research estimates that 5–10% of all Hashimoto’s patients experience persistent symptoms despite normal labs, and since Hashimoto’s itself affects up to 25.8% of women in some populations, that translates to a very large number of people. Many researchers believe the true proportion is even higher, because these patients are so frequently dismissed and never properly counted.
What tests should I be asking for beyond TSH?
A full thyroid panel should include Free T4, Free T3, and TPO antibodies. It’s also worth checking Reverse T3 (rT3), Vitamin D, ferritin, B12, and an inflammatory marker like C-reactive protein (CRP). These tests together paint a far richer picture than TSH alone — and antibody levels in particular can reveal whether active immune activity is driving your symptoms.
What is the T3 conversion problem, and could it apply to me?
Your body converts T4 (the storage form of thyroid hormone) into T3 (the active form that actually runs your metabolism). This conversion requires specific enzymes, and 12–36% of the general population carries a genetic variant that reduces this conversion by about 20%. If you have this variant, your cells may be starved of active T3 even when your TSH and T4 look completely normal — what researchers call tissue-specific hypothyroidism that standard tests cannot see.
Can Hashimoto’s actually cause depression and anxiety?
Yes — and the evidence is striking. A large analysis published in JAMA Psychiatry found that Hashimoto’s patients have 3.5 times higher odds of depression and 2.3 times higher odds of anxiety compared to the general population. The mechanism is neuroinflammation: the same inflammatory cytokines triggered by TPO antibody activity are directly implicated in mood disorders. This is not anxiety caused by being sick — it is a physiological consequence of the autoimmune process itself.
Will selenium supplements actually help me?
The evidence is genuinely encouraging. Multiple large studies have found that selenium supplementation significantly reduces TPO antibody levels, regardless of whether patients are on thyroid hormone therapy. Since lower TPO antibodies mean less immune activation and less inflammatory cytokine production, reducing them is a meaningful therapeutic target. Talk to your provider about whether selenium testing and supplementation make sense for you.
What is thyroidectomy, and why would anyone consider it for ‘normal’ thyroid function?
A thyroidectomy removes the thyroid gland entirely, thereby eliminating the main target of the immune attack—and, with it, the stimulus that triggers the inflammatory process. In the only randomized controlled trial on this question, patients who had thyroidectomy saw their rates of chronic fatigue drop from 82% to 35%, and their general health scores improved by 26 points, while the control group showed no change. It is not a first-line option, but for patients who have suffered for years with no relief from any other approach, it is a legitimate conversation to have with a specialist.
My doctor says my levels are fine and won’t run more tests. What can I do?
Start by clearly documenting your symptoms — their severity, duration, and impact on your daily life — and bring that list to your appointment. You have every right to request a full thyroid panel, including antibodies, and to ask for a referral to a practitioner who specializes in autoimmune thyroid conditions. If your concerns still aren’t addressed, seeking a second opinion is not just acceptable — it’s your right, and it may be the step that finally gets you answers. (Pro tip: Paloma Health has an easy and affordable complete thyroid panel home test kit you can order yourself, as well as access to health care providers with expertise in Hashimoto’s and hypothyroidism.)
Is there anything I can do on my own to feel better while I navigate this?
Absolutely. An anti-inflammatory diet — rich in vegetables, fruits, fatty fish, and olive oil while cutting back on processed foods and refined sugar — directly targets the same inflammatory pathways driving your symptoms. Correcting common deficiencies (Vitamin D, B12, iron/ferritin, zinc) can make a real difference in energy and cognitive function. And because chronic stress powerfully upregulates the same inflammatory signals, prioritizing sleep and stress management is not optional self-care — it is physiologically grounded medicine.



.webp)
%20(1).webp)
.webp)





