
.webp)
In this article
People with hypothyroidism are hearing a lot about GLP-1 and GLP-1/GIP medications like semaglutide and tirzepatide — and for good reason. These medications have changed the conversation around weight loss and type 2 diabetes, but if you live with thyroid disease, the questions are more complicated: Are they safe? Will they affect thyroid hormones? Could they change your dose of thyroid hormone replacement? The answer is yes, they can be an option for many hypothyroid patients — but several important nuances are easy to miss.
For consumers trying to sort through the noise, the key is understanding that GLP-1/GIP medications don’t treat hypothyroidism directly, yet they can still affect thyroid management in practical ways. They may change appetite, body weight, digestion, and sometimes thyroid lab values, which can all influence how a patient feels and how their thyroid medication works. That’s why the smartest approach is not panic, but precision: knowing what these medications do, what they do not do, and what to monitor along the way.
GLP-1 drugs are a class of medications that help lower blood sugar and promote weight loss by mimicking the gut hormone glucagon-like peptide-1; common brand names include Ozempic and Wegovy (semaglutide), Mounjaro and Zepbound (tirzepatide, a dual GIP/GLP-1 drug), Trulicity (dulaglutide), Victoza and Saxenda (liraglutide), Byetta and Bydureon (exenatide), Adlyxin (lixisenatide), and Rybelsus (oral semaglutide), with generic options currently including liraglutide and exenatide in some markets.
GIP refers to glucose-dependent insulinotropic polypeptide, another gut hormone involved in insulin release and blood sugar control; in clinical use, the best-known GIP-related medication is tirzepatide, sold as Mounjaro for type 2 diabetes and Zepbound for weight management, and it is called a dual GIP/GLP-1 receptor agonist because it acts on both pathways.
Weight gain can be one of the most frustrating aspects of hypothyroidism because it often feels like the body is working against you. When thyroid hormone levels are too low, metabolism can slow, energy levels can drop, and the body may burn fewer calories than expected, making it easier to gain weight and harder to lose it. That is one reason GLP-1 and GIP medications have become part of the conversation for some patients: by helping reduce appetite, improve blood sugar control, and support meaningful weight loss, they may offer an added tool for people whose thyroid treatment alone has not solved the weight struggle. For many patients, the challenge is not just the number on the scale — it is the cycle of fatigue, reduced activity, fluid retention, and discouragement that can make healthy habits feel less effective, which is why treating thyroid disease well and considering additional weight-loss support when appropriate can both matter.

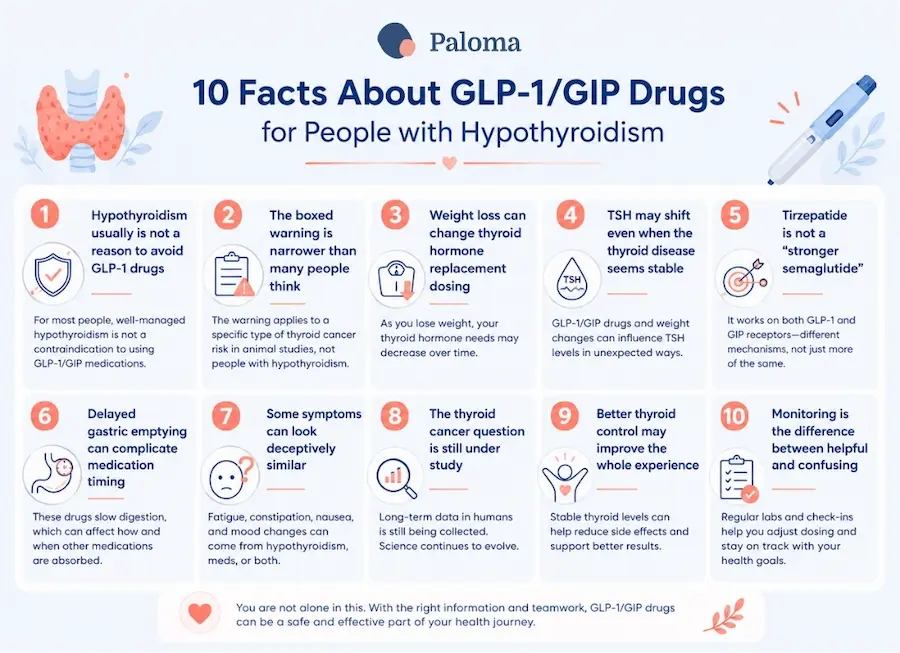
One of the most surprising facts about GLP-1 medications is that hypothyroidism by itself is not typically a reason to avoid them. These drugs are widely used for type 2 diabetes and obesity, and many people with treated thyroid disease can use them safely under medical supervision. The major thyroid-related warning is much narrower: a personal or family history of medullary thyroid carcinoma or MEN2 is the issue of concern, not routine hypothyroidism. That distinction is crucial because the word “thyroid” can lead patients to think that all thyroid conditions are treated the same way.
For consumers, this means the first question is not “Do I have hypothyroidism?” but “What kind of thyroid history do I actually have?” A person whose hypothyroidism is stable on their thyroid hormone replacement medication may still be a candidate for GLP-1 or GLP-1/GIP treatment, especially if obesity or diabetes is also part of the picture. In other words, thyroid disease deserves attention, but it does not automatically close the door.
GLP-1 medications carry a boxed warning that has made many patients uneasy, but the warning is often misunderstood. It was added because rodents developed thyroid C-cell tumors in animal studies, and that raised enough concern to justify a strong warning label. In humans, the concern is focused on medullary thyroid carcinoma, which is rare and biologically distinct from the more common papillary and follicular thyroid cancers.[3][4][6]
That distinction matters because many people hear “thyroid cancer warning” and assume it applies to everyone with a thyroid issue. It does not. The caution is primarily about MTC and MEN2 risk, not about everyday hypothyroidism or even most other thyroid cancers. For patients and clinicians alike, the label should prompt careful screening, not blanket avoidance.[4][3]
A major reason hypothyroid patients need closer monitoring on GLP-1 therapy is that weight loss can alter thyroid hormone requirements. Your dose of thyroid medication is often influenced by body weight, and substantial weight loss can make a previously appropriate dose too strong. That means you may feel fine at first, then later develop symptoms of over-replacement if the dose is no longer matched to your new body size.
This is one of the most practical, relevant things you need to know. The medication may help with weight loss, but your thyroid prescription may need to evolve as your body changes. In one report, patients who lost more than five pounds after starting semaglutide showed reductions in TSH, suggesting that thyroid labs may shift during the early weight-loss phase. The message is simple: when the scale changes, thyroid management may need a fresh look.
You may assume that if you are already taking thyroid medication and feeling reasonably well, your lab values will remain stable. But emerging evidence suggests GLP-1 and GLP-1/GIP therapy may be associated with changes in thyroid function tests in some patients. In a small tirzepatide report, TSH dropped in most participants within a relatively short time after treatment began, prompting the authors to suggest early monitoring. Other studies have also noted thyroid hormone changes in people with obesity who were treated with semaglutide.
These findings do not mean the drugs are damaging the thyroid in a predictable way. They do mean thyroid tests may not be static once treatment begins. A patient can be taking the same dose of thyroid medication and still see a change in TSH because body weight, digestion, and metabolic status are changing in the background. That is one reason thyroid specialists often emphasize follow-up rather than assumptions.
Tirzepatide gets a lot of attention because it combines two actions: GLP-1 and GIP. That dual mechanism helps explain why it can be especially effective for blood sugar control and weight loss. But for hypothyroid patients, the important point is not just that it can be more powerful — it is that it can produce more pronounced downstream changes in appetite, digestion, and weight, all of which can affect your thyroid management.
That makes tirzepatide a little more complicated than a simple “stronger version” of another weight-loss drug. The medication itself does not treat hypothyroidism, but the physiologic changes it triggers can still alter how you experience treatment. That means that thyroid follow-up matters just as much as your choice of GLP-1/GIP drug.

A lesser-known effect of GLP-1 medications is that they slow gastric emptying, which is part of how they help people feel full longer. That slowing can be helpful for weight loss, but it may also affect the absorption of oral medications, including thyroid medication, in some patients. In practical terms, that means the “same” thyroid pill may not behave exactly the same way once a GLP-1 medication is introduced.
This does not mean that your thyroid hormone replacement stops working. It means you and your health care provider need to watch for changes in thyroid levels or symptoms and adjust as needed. For patients, it is smart to keep taking thyroid medication consistently, on schedule, and to report any new symptoms after starting GLP-1/GIP therapy. When a medication changes the pace of digestion, absorption can become part of the story.
One of the biggest frustrations for patients is that GLP-1 side effects can overlap with hypothyroid symptoms. Nausea, constipation, fatigue, and reduced appetite are common complaints with these medications, and several of them can also show up when your thyroid hormone is not optimized. That overlap can make it difficult to tell whether you’re experiencing medication adjustment issues, under-treated hypothyroidism, or simply the expected early side effects of treatment.
This is why symptom tracking matters. If you feel unusually tired after starting a GLP-1 medication, the answer is not always “your thyroid is off.” It could be the drug itself, reduced calorie intake, dehydration, or a real thyroid dose mismatch. A careful review of symptoms, labs, and medication timing often gives the clearest answer.

The thyroid cancer concern around GLP-1 therapy has attracted a lot of headlines, but the human data have been more reassuring than the animal data that triggered the warning. Several analyses have not found a significant overall increase in thyroid cancer risk, and newer reviews suggest that some early diagnoses may reflect detection bias rather than a true causal effect. A Mayo Clinic summary of recent findings reported that the pattern may be explained by more frequent medical surveillance in people who start these medications.
Even so, researchers are still studying the question, and that is why clinicians continue to treat the boxed warning seriously in patients with medullary thyroid cancer risk. For consumers, the take-home message is balanced: there is enough reassurance to support use in appropriate patients, but not enough reason to dismiss the warning entirely. That middle ground is often the most medically honest place to be.
When you’re hypothyroid, it’s easy to feel discouraged by weight struggles, and that can make GLP-1 medications especially appealing. But the best outcomes usually come when thyroid replacement is already optimized, not when it is left to drift. If you’re under-replaced and undertreated before starting treatment, you may feel like the new medication is “not working” when the real issue is that the thyroid itself still needs adjustment.
That is one reason many clinicians prefer to confirm stable thyroid function before or soon after initiating a GLP-1 or GLP-1/GIP medication. When thyroid levels are in range, the benefits of appetite suppression and metabolic improvement may be easier to see. Think of it as reducing background noise so the medication’s real effect is easier to measure.
The most important surprise may be that the medications themselves are only part of the story. For hypothyroid patients, the real key is monitoring — especially during active weight loss, dose escalation, or symptom changes. That may include checking your thyroid levels after significant weight loss, reviewing the timing of your thyroid medication, and paying attention to side effects that seem out of proportion.[9][10][14][7]
This is especially important because a good experience on GLP-1 or GIP therapy can suddenly turn confusing if your thyroid dosing is no longer aligned with your body. The fix is often straightforward, but only if the problem is recognized early. Regular follow-up makes a potentially messy transition manageable.
Before starting a GLP-1 or GLP-1/GIP medication, you should ask whether your thyroid disease is stable, whether you have any personal or family history of medullary thyroid carcinoma or MEN2, and when your next thyroid labs should be checked. It is also wise to ask whether the timing of your levothyroxine or natural desiccated thyroid should be reviewed if nausea or reduced appetite make morning routines more difficult. Those conversations may seem small, but they can prevent a lot of confusion later.[3][4][6][14][9]
The goal is not to create fear around an effective class of medications. It is to make sure thyroid disease is part of the prescribing conversation from the beginning, not an afterthought once symptoms shift. For many hypothyroid patients, that more careful approach is what makes the medication both usable, useful, and ultimately successful for you.
GLP-1 and GLP-1/GIP medications can be appropriate for many people with hypothyroidism, but they are not a one-size-fits-all solution. The biggest issues are not whether you are hypothyroid, but whether you have rare thyroid cancer risks, whether your thyroid hormone dose remains appropriate, and whether your thyroid labs are monitored as weight changes. In short, these medications can fit into your thyroid care — but they work best when your thyroid care is carefully and actively managed alongside them.
That is actually good news. It means hypothyroidism does not automatically shut the door on a promising treatment, and it also means there are clear ways to use these drugs more safely and intelligently. With the right follow-up, the combination of thyroid care and GLP-1/GIP therapy can be practical, effective, and transparent.
You can rely on Paloma Health to help you manage your thyroid and GLP-1/GIP treatment together with more confidence. As your weight changes, your thyroid hormone needs may change too, and Paloma can help you stay on top of lab monitoring with convenient home thyroid testing, symptom checks, and medication adjustments so your treatment plan keeps up with your body’s changes. That means you’re less likely to confuse GLP-1/GIP side effects like nausea, constipation, or fatigue with thyroid symptoms, and you have the Paloma team looking at the full picture rather than treating each issue separately.
Can people with hypothyroidism take GLP-1 medications?
Yes. Most people with treated hypothyroidism can safely use GLP-1 or GLP-1/GIP medications under medical supervision, provided they do not have certain rare thyroid cancer risks.
Do GLP-1 medications treat hypothyroidism?
No. These medications are designed to help with weight loss and blood sugar control, not to replace thyroid hormone or treat an underactive thyroid.
Why do GLP-1 medications carry a thyroid warning?
The warning is based on animal studies that showed thyroid C-cell tumors in rodents. In humans, the concern is primarily limited to people with a personal or family history of medullary thyroid carcinoma or MEN2.
Can weight loss change my thyroid medication dose?
Yes. Significant weight loss can alter your body’s thyroid hormone requirements, meaning your thyroid medication dose may need to be adjusted over time.
Can GLP-1 medications affect thyroid blood test results?
They can. Some studies have found changes in TSH levels after starting GLP-1 or GLP-1/GIP therapy, which is why follow-up testing is important.
Is tirzepatide the same as semaglutide?
No. Tirzepatide acts on both GIP and GLP-1 receptors, while semaglutide acts only on GLP-1 receptors, leading to somewhat different effects.
Can GLP-1 medications affect how my thyroid medicine is absorbed?
Possibly. Because these medications slow stomach emptying, they may affect the absorption of some oral medications, including thyroid hormone replacement.
How can I tell whether symptoms are from my thyroid or the GLP-1 medication?
It can be difficult because symptoms such as fatigue, constipation, and changes in appetite can occur with both. Tracking symptoms and checking thyroid labs can help identify the cause.
Do GLP-1 medications increase thyroid cancer risk?
Current human research has been largely reassuring and has not shown a significant overall increase in thyroid cancer risk. However, researchers continue to study the issue, and the boxed warning remains important for people with specific risk factors.
What should I discuss with my healthcare provider before starting a GLP-1 medication?
Ask whether your hypothyroidism is well controlled, whether you have any thyroid cancer risk factors, and when your thyroid labs should be checked after starting treatment. You should also discuss whether changes in weight or digestion could affect your thyroid medication routine.



.webp)

%20(1).webp)





