
.webp)
In this article
The sensation can start small and then take over. One day, you notice a strange sensation of searing heat in your tongue, a stinging sensation in your lips, or your mouth feels like it has been scalded by something too hot. Days or weeks later, the feeling may be constant, exhausting, and impossible to ignore. Burning mouth syndrome can be one of the most unsettling oral pain conditions because your mouth can look completely normal, even while your discomfort is intense.
That disconnect is part of what makes burning mouth syndrome so frustrating. Sufferers often bounce between dentists, primary care clinicians, and specialists before they get an explanation, and even then, the answer is often not simple. Many medical professionals treat oral pain as a localized dental problem, but burning mouth syndrome is not a single disease with a single cause. It's actually a syndrome with multiple possible drivers. Some cases are primary, meaning there is no clear underlying cause; others are secondary, meaning the burning is linked to another condition such as thyroid disease, a nutritional deficiency, dry mouth, medication effects, oral infection, or hormonal changes.
Burning mouth syndrome symptoms usually include a burning, scalding, tingling, or hot sensation involving the tongue, lips, gums, palate, cheeks, roof of the mouth, or the entire mouth. Many people also report dry mouth, altered taste, or a persistent metallic or bitter flavor. Symptoms may be worse in the afternoon or evening, and they can wax and wane in severity from day to day.
The pain can affect much more than eating or drinking. For some people, it changes how they sleep, socialize, and work, especially if the discomfort makes spicy, acidic, crunchy, or hot foods intolerable. Because the condition is invisible to others, it can also be emotionally draining, leading to anxiety, frustration, or a sense of being dismissed.
There is still no single explanation for burning mouth syndrome. Many experts believe primary burning mouth syndrome is a neuropathic pain disorder, meaning the nerves that carry pain signals may become overly sensitive or misfire even when there is no obvious injury. That helps explain why the mouth can feel inflamed or burned even when the tissues look normal.
Secondary burning mouth syndrome is different. In these cases, the burning is a symptom of something else, and the key is finding that root cause. Common contributors include dry mouth, oral candidiasis (yeast overgrowth), iron deficiency, low vitamin B12, folate or zinc deficiency, diabetes, reflux, medication side effects, contact irritation from oral products, autoimmune disease, and thyroid abnormalities.
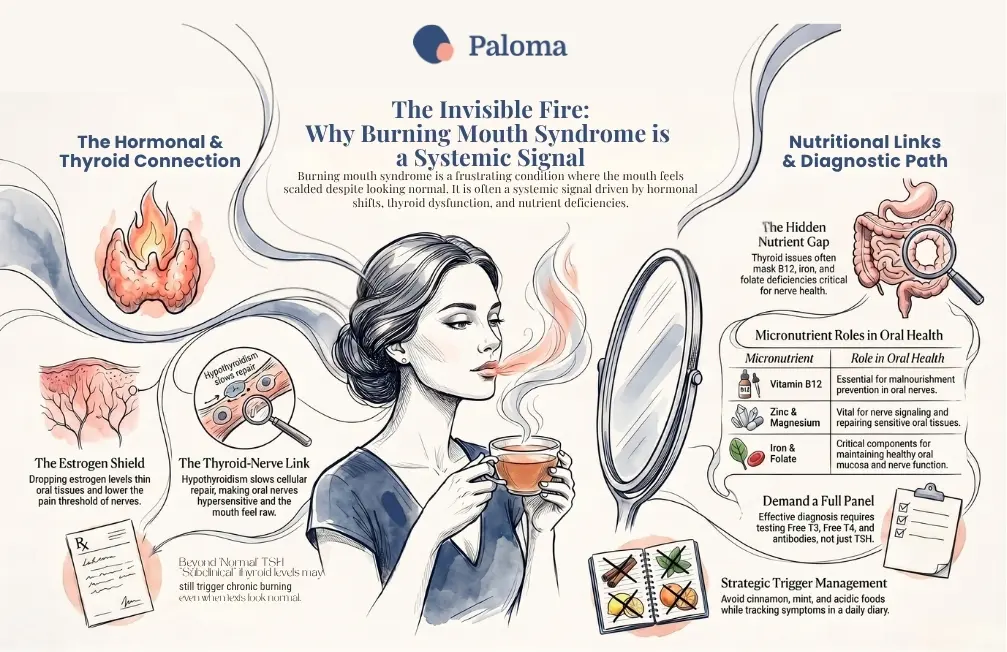
Estrogen acts as a protective agent for your oral cavity, influencing the density of the skin cells and the function of salivary glands. High-quality saliva is essential for buffering acidity and protecting your oral nerves. When estrogen levels fluctuate, the mucosa can become thin, dry, and hypersensitive. This physiological shift significantly alters your oral environment, transforming it into a high-friction zone where even minor sensations can cause painful oral symptoms.
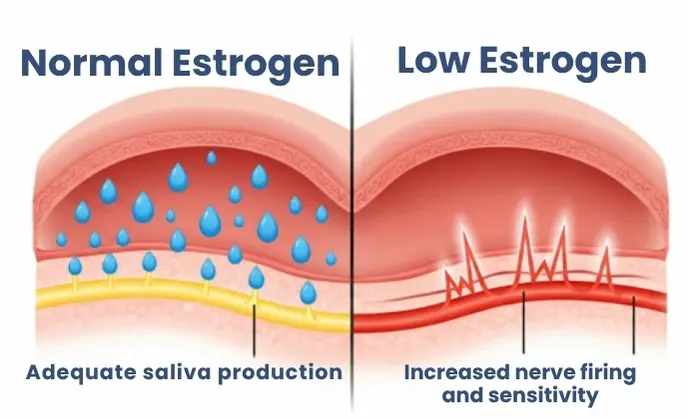
How estrogen depletion alters the oral environment: A drop in hormones thins the protective mucosa, reduces saliva production, and lowers the pain threshold of the lingual nerve, triggering burning mouth syndrome symptoms.
The neurological link: How hormonal fluctuations sensitize the lingual nerve
The lingual nerve, which provides sensation to your tongue, is highly responsive to hormonal shifts. Estrogen and progesterone affect neurosteroids that govern pain processing. When these hormones drop, the "threshold" for nerve firing often lowers, making the nerve very excitable. This hypersensitivity is a core component of burning mouth syndrome, often appearing as a spontaneous, chronic pain and other oral symptoms that don't respond to typical pain relief.
The Hashimoto's connection
Hashimoto's thyroiditis is an autoimmune condition that often leads to hypothyroidism, and thyroid disease is one of the systemic problems repeatedly associated with burning mouth syndrome. Research has found links between burning mouth symptoms and thyroid dysfunction, including studies specifically examining people with Hashimoto's thyroiditis.
That does not prove that Hashimoto's thyroiditis directly causes burning mouth syndrome, but it does mean that thyroid evaluation is important when someone presents with unexplained oral burning. Thyroid conditions may contribute to symptoms such as altered taste, dry mouth, or autoimmune overlap, and health care providers should include thyroid testing as part of the workup for persistent mouth burning.
Hypothyroidism and burning mouth syndrome
The thyroid gland acts as the body's metabolic thermostat. When it slows down, every cell in the body receives less energy to perform repair and maintenance, including the delicate cells of the oral lining. A low metabolic state often leads to a sluggish immune response, making the mouth more susceptible to burning and dryness.
Hypothyroidism may show up in the mouth in ways that are easy to miss: dry mouth, altered taste, and burning discomfort. Reduced thyroid function can affect saliva, nerve signaling, and oral tissue sensitivity, among other symptoms. All of these symptoms can make your mouth feel raw or irritated, even when it appears normal.
For patients with known hypothyroidism, new oral burning symptoms should not be ignored as "just part of thyroid disease." They may reflect undertreatment, another nutritional or autoimmune issue, medication side effects, or true burning mouth syndrome. That is why thyroid testing is one piece of the diagnostic process, rather than the complete answer.
Why "subclinical" thyroid issues may still cause chronic burning
Many healthcare providers rely on a narrow range for thyroid-stimulating hormone (TSH) testing, often ignoring "subclinical" levels that fall outside the optimal range. However, for a patient with burning mouth syndrome, these borderline values are significant. A patient's unique physiology might require a tighter, more optimized range to prevent symptoms, and ignoring these subtle shifts is a common failure in the current standard of care.
Burning mouth syndrome occurs far more frequently in women, particularly during perimenopause and menopause. Researchers believe this is largely due to declining estrogen and other reproductive hormones that help maintain oral tissue health, support saliva production, and regulate nerve function. During the menopausal transition, hormonal changes often coincide with sleep disruption, stress, medication use, reflux, and dry mouth—creating a perfect storm for oral discomfort.
As hormone levels fluctuate and eventually decline, the mouth may become drier and more sensitive, while pain pathways become more reactive. The result can be a persistent burning, tingling, or scalding sensation affecting the tongue, lips, palate, or other areas of the mouth. Studies show that symptoms often first appear—or become significantly worse—during perimenopause and menopause, yet oral complaints are frequently overlooked compared with more familiar symptoms such as hot flashes and night sweats. Many women report oral burning, altered taste, or increased mouth sensitivity years before their final menstrual period.
The hormonal connection is further supported by prevalence data showing that women are significantly more likely than men to develop burning mouth syndrome, with rates peaking in the years immediately after menopause. Some studies suggest that appropriately managed hormone replacement therapy may reduce symptoms in certain women, although results vary. While symptoms may improve once hormone levels stabilize, others require ongoing treatment. For this reason, menopausal status should be considered when evaluating burning mouth syndrome, particularly in women with dry mouth, taste disturbances, or coexisting conditions such as autoimmune thyroid disease.

There is no one definitive test for burning mouth syndrome. Instead, diagnosis usually begins with a careful history and physical exam, followed by testing to rule out other conditions that can cause similar symptoms. Mayo Clinic notes that clinicians commonly review medical history and medicines and may order blood tests to assess blood sugar, thyroid function, nutritional factors, and immune system function.
The workup may also include looking for oral infection, dry mouth, reflux, allergy, or irritation from toothpaste or dental materials, and side effects from medications that can reduce saliva or irritate oral tissues. If the mouth exam is normal and other causes are excluded, a clinician may diagnose primary burning mouth syndrome. If another condition is found, treatment is directed at that underlying issue.
Thyroid testing
Thyroid evaluation should be part of a workup for burning mouth syndrome, but you should be aware that a standard thyroid stimulating hormone test is insufficient. To truly address the problem, you need a full panel, including free triiodothyronine (free T3), free thyroxine (free T4), thyroid antibody tests, and reverse T3, in addition to the TSH test. Similarly, sex hormones like estradiol and progesterone should be checked at specific times in the cycle or, if post-menopausal, via blood or saliva monitoring to understand the full hormonal landscape.
A symptom diary and medical history
You should create a detailed symptom diary. By tracking food, stress levels, hormonal cycles, and even weather changes, you can create a data set that helps identify personal triggers. This objective data is a powerful tool to share with your care providers.
Also, take the time to review your medical history for patterns. Did the burning start after a stressful event, a change in medication, or during a shift in your hormonal health? Being your own health historian is the best way to prepare for a successful interaction with your healthcare provider.
Treatment depends on whether the condition is primary or secondary. For secondary burning mouth syndrome, addressing the cause may ease symptoms: correcting nutritional deficiencies, treating oral infections, adjusting medications that cause dry mouth, or managing your thyroid dysfunction can all make a difference.
Primary burning mouth syndrome is harder to treat because there is no known cure and no universally effective therapy. Mayo Clinic lists saliva replacement products, specific oral rinses or lidocaine, capsaicin, alpha-lipoic acid, clonazepam, certain antidepressants, medications that block nerve pain, and cognitive behavioral therapy among treatment options. The best choice often depends on the symptom pattern and the individual patient's response.
Some nonprescription strategies can also help. People are often advised to drink plenty of fluids, suck on ice chips, avoid alcohol and tobacco, limit acidic or spicy foods, avoid cinnamon and mint if those trigger symptoms, use mild or flavor-free toothpaste, and reduce stress where possible. These steps do not cure the condition, but they can reduce triggers and improve day-to-day comfort.
Burning mouth syndrome can be difficult to describe to other people, and that alone can make it isolating. Because there may be no visible sign of damage, patients sometimes worry that their symptoms will be minimized or misattributed to stress alone. But the condition is well recognized in dental and medical literature, and the pain is real.
The most practical approach is usually a combination of diagnosis, trigger management, and symptom control. Many patients need to try more than one treatment before finding the right mix, and progress can be gradual rather than immediate. The goal is not just to reduce pain, but to help people eat, speak, sleep, and live more comfortably.
Why thyroid issues often mask B12, iron, and folate deficiencies
Thyroid dysfunction often impairs the absorption of essential nutrients, such as vitamin B12, iron, and folate. These nutrients are critical for nerve health. If a patient's B12 is low, the nerves in the mouth become malnourished, leading to burning. Providing supplemental support for these deficiencies is often the "missing link" in treatment.
The role of zinc and magnesium in nerve regeneration
Zinc and magnesium are vital for nerve signaling and tissue repair. Many of our food systems have become depleted of these minerals, and hormonal imbalances further deplete our existing stores. Ensuring adequate intake of these nutrients can provide the essential building blocks the body needs to heal hypersensitive oral nerves.
Healthy eating vs. targeted nutrition: Adjusting food choice for nerve support
Transitioning from general "healthy eating" to targeted nutrition is key. This means prioritizing anti-inflammatory fats, high-quality proteins for collagen support, and avoiding trigger foods like spicy or highly acidic items that may aggravate the already sensitive oral mucosa.
Anyone with persistent mouth burning lasting more than a couple of weeks should see a dentist or clinician, especially if dry mouth, taste changes, weight loss, oral lesions, or signs of thyroid or autoimmune disease accompany the symptoms. The earlier the evaluation, the sooner treatable causes can be found and addressed.
For women in perimenopause or menopause, and for patients with Hashimoto's or hypothyroidism, it is especially important not to assume the problem is harmless or purely hormonal. Burning mouth syndrome may be related to hormones, but it may also be a clue to a fixable medical problem that deserves a proper workup.

Burning mouth syndrome is not merely a "mouth issue"—it is a systemic signal that your hormones, thyroid, or nutritional status are out of balance. The path to relief starts with acknowledging that your pain is real, even when standard tests suggest otherwise. By shifting your perspective toward an integrated, data-driven approach, you can bridge the gap between "normal" results and actual health.
To move forward, begin by reviewing your recent health history and requesting a comprehensive evaluation that goes beyond basic screening tests. Because thyroid dysfunction, autoimmune thyroid disease, nutrient deficiencies, and hormonal fluctuations can all contribute to burning mouth syndrome, a thorough assessment is essential. Paloma Health makes this process easier with its convenient at-home thyroid test kit, which measures key thyroid markers including TSH, free T4, free T3, and thyroid antibodies. Combined with access to specialized thyroid care providers, personalized treatment plans, symptom-tracking tools, and ongoing virtual support, Paloma helps patients identify and address root causes rather than simply manage symptoms.
Advocate for yourself by building a collaborative healthcare team and tracking changes in your symptoms over time. Whether your burning mouth syndrome is linked to thyroid disease, menopause, nutritional deficiencies, or another underlying condition, identifying and treating the underlying cause can make a meaningful difference. While the medical community continues to learn more about this complex condition, taking a proactive approach to your thyroid and hormonal health today may help extinguish the fire and restore the comfort, confidence, and quality of life you deserve.
.webp)
Limited offer
20% off your first Thyroid Test
What is burning mouth syndrome?
Burning mouth syndrome is a chronic condition that causes a burning, tingling, or scalding sensation in the mouth despite the absence of visible injury or irritation. Symptoms can affect the tongue, lips, gums, palate, or the entire mouth.
What does burning mouth syndrome feel like?
People often describe it as a sensation similar to having burned their mouth on hot food or beverages. It may also be accompanied by dryness, numbness, tingling, or a metallic or bitter taste.
Can hypothyroidism cause burning mouth syndrome?
Hypothyroidism has been linked to burning mouth symptoms in some people. Reduced thyroid function may contribute to dry mouth, altered taste perception, increased nerve sensitivity, and changes in oral tissues.
Is Hashimoto's disease associated with burning mouth syndrome?
Research suggests an association between Hashimoto's thyroiditis and burning mouth syndrome. While Hashimoto's may not directly cause the condition, thyroid evaluation is an important part of the diagnostic process.
Why is burning mouth syndrome common during menopause?
Declining estrogen levels can reduce saliva production, thin oral tissues, and increase nerve sensitivity. These changes may make women in perimenopause and menopause more susceptible to oral burning symptoms.
Can vitamin deficiencies cause a burning sensation in the mouth?
Yes. Deficiencies in vitamin B12, iron, folate, zinc, and other nutrients have been associated with burning mouth symptoms because they affect nerve health and tissue repair.
How is burning mouth syndrome diagnosed?
There is no single test that confirms the diagnosis of burning mouth syndrome. Diagnosis typically involves ruling out other possible causes through medical history, oral examination, blood tests, and evaluation of thyroid, nutritional, hormonal, and autoimmune factors.
What tests should I ask for if I have burning mouth symptoms?
In addition to a dental evaluation, consider discussing thyroid testing, blood sugar screening, and assessments for vitamin and mineral deficiencies with your healthcare provider. Hormone testing may also be appropriate for women in perimenopause or menopause.
What treatments are available for burning mouth syndrome?
Treatment depends on the underlying cause. Options may include correcting nutritional deficiencies, treating dry mouth or infections, optimizing thyroid function, avoiding triggers, and using medications or therapies that help manage nerve-related pain.
When should I see a healthcare provider about burning mouth symptoms?
You should seek evaluation if burning symptoms persist for more than a few weeks or interfere with eating, speaking, or sleeping. Early assessment can help identify potentially treatable causes and prevent unnecessary suffering.


%20copy.webp)
%20copy%202.webp)







