
.webp)
In this article
Testosterone is men’s primary sex hormone and anabolic steroid, serving an essential role in male development. While we strongly associate testosterone with men, it is also present in females, and both sexes can experience problems when testosterone levels are low.
If you have hypothyroidism, the most common thyroid disease, you need to understand the effect that your thyroid can have on testosterone levels. Low thyroid function can disrupt the hormone systems that help regulate testosterone, and that can show up as fatigue, low libido, mood changes, erectile dysfunction, reduced muscle mass, and “not feeling like yourself” symptoms.
The catch is that low thyroid hormone levels and low testosterone often look a lot alike. That overlap matters, because a person can spend months chasing one hormone issue when the real problem is an underactive thyroid — or, in some cases, both.
The thyroid is a small gland with a big job. It produces thyroid hormones, which help regulate metabolism, energy production, body temperature, digestion, and much more. When thyroid hormones are too low, many body systems slow down at once.
Testosterone is also part of a larger endocrine network, not a standalone hormone. In men, it is produced mainly in the testes, while women make smaller amounts in the ovaries and adrenal glands; both sexes depend on the hypothalamic-pituitary-gonadal axis, which can be influenced by thyroid hormone status.
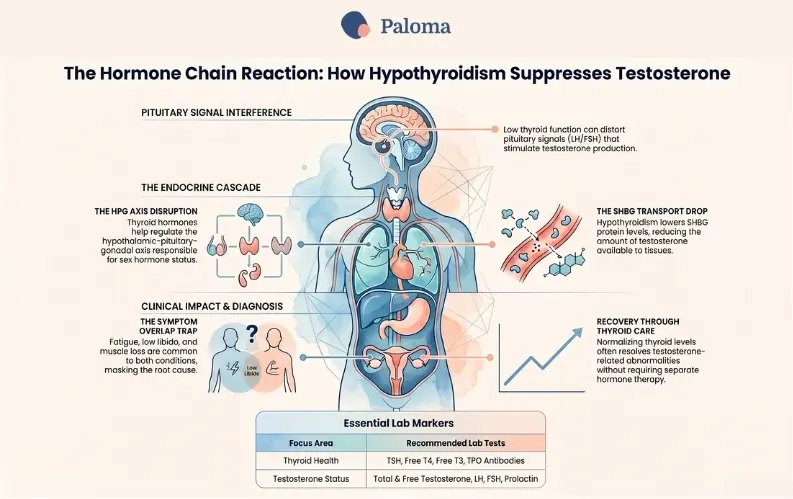
That is why thyroid conditions can ripple outward into changes in sex hormones. When thyroid function drops, the brain and body may send weaker or distorted signals to hormone-producing organs, and testosterone can fall as part of that chain reaction.
Hypothyroidism occurs when your thyroid gland does not produce enough thyroid hormone to support normal body function. In practical terms, that means your body’s “pace” slows down, and everyday activities may feel harder than they should.
Common hypothyroidism symptoms include fatigue, cold intolerance, constipation, depression, muscle aches, joint pain, a slow heartbeat, and sexual dysfunction. Because these symptoms are broad and nonspecific, hypothyroidism is easy to miss or dismiss as stress, aging, burnout, or poor sleep.
One of the most common causes of hypothyroidism is Hashimoto’s disease, an autoimmune condition in which the immune system attacks your thyroid gland. Over time, that damage can reduce the gland’s ability to make thyroid hormone.
Other causes include
- Hashimoto’s disease: Sometimes, the immune system, meant to protect the body from invading infections, mistakenly identifies the thyroid gland as “foreign,” and attacks. If there is significant damage, the thyroid gland may no longer produce enough thyroid hormone, leading to hypothyroidism.
- Surgical removal of part or all of the thyroid gland: People with thyroid nodules, thyroid cancer, or Graves’ disease may need to have part or all of their thyroid removed, causing hypothyroidism. If the gland is only partially removed, the body may still be able to make enough thyroid hormone on its own.
- Radiation treatment: People with Graves’ disease, nodular goiter, or thyroid cancer may be treated with radioactive iodine to destroy the thyroid gland. Radiation treatment may also be used on patients with Hodgkin’s disease, lymphoma, or cancers of the head or neck. These patients may lose part or all of their thyroid function, causing hypothyroidism.
- Congenital hypothyroidism: Congenital hypothyroidism is a partial or complete loss of function of the thyroid gland that affects infants from birth. Congenital hypothyroidism is caused by the baby not getting enough iodine in the womb or thyroid gland damage or malformation.
- Certain medications: Medicines like amiodarone, lithium, interferon-alpha, and interleukin-2 can prevent the thyroid gland from being able to produce hormones. These drugs may trigger hypothyroidism in patients with a genetic predisposition to autoimmune thyroid disease.
- Too much or too little iodine: The thyroid gland needs iodine from food to produce thyroid hormones. However, taking too much iodine can cause or worsen hypothyroidism. Iodine deficiency is not typically an issue in the United States because salt is iodized.
- Damage to the pituitary gland: The pituitary gland (or the “master gland”) instructs the thyroid on how much hormone to make. The pituitary gland may no longer be able to communicate correctly with the thyroid gland if it is damaged by a tumor, radiation, or surgery, possibly leading to hypothyroidism.
The cause matters because it can shape treatment, follow-up, and whether other hormone systems are affected, too.
The relationship between thyroid function and testosterone is not just theoretical. Thyroid hormone helps regulate the organs and signaling pathways involved in sex hormone production, and researchers have repeatedly found that hypothyroidism can alter testosterone-related measures.
One key player is sex hormone-binding globulin, known as SHBG. SHBG is a protein produced by the liver that binds testosterone, dihydrotestosterone, and estrogen, helping regulate the amount of each hormone available to tissues.
When thyroid activity is low, SHBG often decreases. That can reduce total testosterone and, in some cases, free testosterone as well, depending on the rest of the hormonal picture.
Thyroid dysfunction can also affect luteinizing hormone and follicle-stimulating hormone, the pituitary signals that help stimulate testosterone production. In other words, the problem may not be confined to the thyroid itself; it can affect the whole hormonal conversation.
Several clinical studies and reviews support a connection between hypothyroidism and lower testosterone. Older studies found that men with hypothyroidism had lower total testosterone and SHBG, and that thyroid hormone treatment increased SHBG and helped normalize testosterone values.
A later review on thyroid function, sex hormones, and sexual function reported that thyroid hormone replacement in hypothyroid patients can bring SHBG, free testosterone, and prolactin back toward normal and resolve sexual dysfunction. That is an important point: the hormonal imbalance may improve when the thyroid is treated, without the need for separate testosterone therapy.
A broader review of thyroid dysfunction and sexual function reached a similar conclusion, finding that sexual problems often improve after thyroid correction, especially in men with erectile dysfunction and other symptoms. More recent research continues to show associations between hypothyroidism and sex hormone changes in both men and women.
This is where things get tricky. Low thyroid and low testosterone can feel almost interchangeable in everyday life.
In men, common symptoms of low testosterone include reduced sexual desire, erectile dysfunction, loss of muscle mass, weight gain, fatigue, depressed mood, irritability, and hair loss. Those same complaints can also show up in hypothyroidism, which means a person can easily be misdiagnosed if only one hormone is checked.
In women, testosterone is less discussed but still important. Research is smaller and less definitive, yet low testosterone in women has been linked to low libido, depressed mood, muscle weakness, and changes in sexual responsiveness. Hypothyroidism can also contribute to sexual discomfort and reduced interest in sex, making the picture even more complex.

Most of the strongest testosterone-thyroid research has been done in men, so there is more certainty about how hypothyroidism affects male testosterone than female testosterone. That said, women are not exempt from the hormone relationship.
Women naturally have much lower testosterone levels than men, so even modest changes can be meaningful. Newer research suggests thyroid disorders are associated with a sexual dysfunction in women, including reduced sex drive and discomfort during sex.
One recent review found that sexual dysfunction was common among women with thyroid disorders, with notable prevalence in women with hypothyroidism. While that does not prove testosterone is the only mechanism, it reinforces the idea that thyroid disease can affect sexual health in ways that are easy to overlook.
SHBG may sound like just another acronym, but it helps explain why thyroid disease changes hormone results. It acts as a transport protein that binds hormones and influences how much is available for the body to use.
In hypothyroidism, SHBG often falls. That can alter total testosterone readings and sometimes mask the real issue, especially if a clinician only looks at one number without considering free testosterone, symptoms, and thyroid labs together.
There is also the flip side: in hyperthyroidism, SHBG tends to rise, which can increase total testosterone while free testosterone remains normal or lower than expected. That contrast helps show that thyroid status strongly shapes the interpretation of sex hormones.
Sometimes low thyroid and low testosterone share a deeper root cause. The pituitary gland helps regulate both systems, so if it is not functioning properly, thyroid and testosterone signaling can be affected.
That is why experts recommend looking beyond the gonads when testosterone is low. A review on testosterone replacement therapy and endocrine evaluation notes that clinicians should consider pituitary and thyroid dysfunction, and that checking thyroid function can be especially enlightening in men with hypogonadism.
This matters because a person may appear to have a straightforward testosterone problem when the real issue is secondary hypogonadism, pituitary disease, or a broader endocrine disorder. Treating the visible symptom without finding the upstream cause is often a dead end.
If symptoms suggest both thyroid and testosterone issues, a more comprehensive blood test workup is often the best approach. For thyroid, that usually includes a complete thyroid function test that evaluates thyroid-stimulating hormone (TSH), free T4, free T3, and thyroid peroxidase (TPO) antibodies, especially if Hashimoto’s disease is suspected.
.webp)
Limited offer
20% off your first Thyroid Test
For testosterone concerns, clinicians commonly order total testosterone, free serum testosterone, luteinizing hormone (LH), follicle-stimulating hormone (FSH), and, sometimes, prolactin. The combination of these results can help determine whether the problem is coming from the thyroid, pituitary, testes, or ovaries, or several places at once.
A single abnormal result rarely tells the whole story. Hormone testing works best when interpreted in context, because age, sleep, stress, obesity, medications, and chronic illness can all influence the results.
The main treatment for hypothyroidism is thyroid hormone replacement, taken daily. When thyroid levels are restored, related hormone abnormalities may improve too, including testosterone-related measures.
That is one reason clinicians are careful about jumping straight to testosterone therapy. If low testosterone is partly caused by untreated hypothyroidism, correcting the thyroid disorder may relieve symptoms and normalize hormone balance without additional treatment.
Testosterone replacement therapy is most clearly indicated for primary hypogonadism, when the testes cannot make enough testosterone. It is sometimes marketed more broadly for energy, vitality, and aging, but the evidence for those uses is much less solid.
Testosterone therapy can be helpful in the right patient, but it is not a universal fix for fatigue or low sex drive. If the true driver is thyroid disease, low iron, depression, sleep apnea, or another medical issue, testosterone alone may not address the problem.
There are also tradeoffs. Testosterone therapy can worsen acne, contribute to sleep apnea, affect fertility, and raise concerns about prostate growth or other complications in some patients. That is why a thorough evaluation matters before starting treatment.
The thyroid-testosterone connection is not just about lab values. It affects real life: intimacy, mood, energy, confidence, and relationships.
In men, hypothyroidism is often associated with erectile dysfunction, low desire, and diminished sexual satisfaction. In women, thyroid disorders have been linked to reduced libido, vaginal dryness, and broader sexual dysfunction.
Because sexual symptoms can have emotional consequences, people may blame themselves or assume the problem is psychological. In reality, a biological cause like hypothyroidism and issues with your hormonal balance may be contributing, and that is something worth checking.
If you have symptoms like low energy, brain fog, low libido, erectile dysfunction, unexplained weight gain, muscle loss, or mood changes, it is reasonable to think bigger than one hormone.
A thyroid evaluation can be especially useful if you have never been tested, have a family history of autoimmune disease, or have other signs like constipation, cold intolerance, or dry skin. If the thyroid is off, testosterone may be part of the story — but it may not be the whole story.
At Paloma, we know that your thyroid health and testosterone status often go hand in hand. When symptoms like fatigue, low libido, weight changes, mood shifts, or brain fog show up, it is important to look at the whole hormonal picture — not just one lab value or one diagnosis.
That is why Paloma takes a comprehensive approach, evaluating thyroid function with appropriate thyroid tests and considering how low thyroid hormone levels may be affecting testosterone and other hormones. By identifying the root cause, we can create a treatment plan that is designed to support lasting relief, better energy, and improved quality of life.
Paloma makes it easier to get expert care, home testing, personalized treatment, and ongoing support from clinicians who understand the connection between thyroid disorders and hormone balance. Paloma is built to help you address your hormonal health thoughtfully and effectively — so you can feel like yourself again.
Can hypothyroidism cause low testosterone?
Yes. Low thyroid hormone can reduce testosterone availability and disrupt the signals that help regulate sex hormone production.
Will treating hypothyroidism raise testosterone?
Often it will help. Research shows that thyroid hormone replacement can normalize SHBG, free testosterone, and sexual symptoms in many patients.
Why do hypothyroidism and testosterone deficiency feel so similar?
They overlap because both can cause fatigue, low mood, reduced sex drive, weight gain, and muscle loss. That is why one condition can be mistaken for the other.
Should thyroid tests be part of a low testosterone workup?
Yes, especially if symptoms are broad or the cause is unclear. Thyroid testing can reveal a treatable problem that would otherwise be missed.
What thyroid tests are most useful?
TSH, free T4, free T3, and TPO antibodies are commonly used. TPO antibodies are especially helpful when Hashimoto’s thyroiditis is suspected.
Does hypothyroidism affect women’s testosterone, too?
Yes, although the research base is smaller than it is for men. Women with thyroid disorders can also experience sexual dysfunction and hormone changes.
What is SHBG?
SHBG is a liver-made protein that binds hormones such as testosterone and estrogen and affects how much is available to the body. Thyroid function strongly influences SHBG levels.
Is testosterone replacement a substitute for thyroid treatment?
No. If hypothyroidism is the underlying problem, treating the thyroid is usually the first priority. Testosterone therapy may have a role later, but it should not replace proper thyroid care.
If you want, I can next turn this into a polished SEO-ready article with a stronger headline, subhead suggestions, meta description, and internal-link placements for Paloma Health.

%20copy%202.webp)



%20(1).webp)





