
.webp)
In this article
Meet the expert
Nina Mosier, M.D. is a retired internist and Co-Founder & Executive Director of Power for Parkinson's, an organization dedicated to support for Parkinson's patients. Power for Parkinson's also runs a popular YouTube channel featuring a schedule of live and recorded exercise classes.
If you live with Hashimoto's thyroiditis or hypothyroidism, you probably already know the feeling: a brain that moves through molasses, a body that won't cooperate, muscles that ache and stiffen, a kind of slowness that no amount of rest seems to fix. You've likely been told it's "just" your thyroid. But what if some of those symptoms — a tremor, shuffling gait, frozen expression, and cognitive fog — had a deeper, neurological dimension? What if your thyroid condition was quietly affecting your brain in ways your doctors haven't yet connected?
An expanding body of research is drawing a striking map between thyroid dysfunction — particularly autoimmune thyroid disease like Hashimoto's — and the neurological world of Parkinson's disease and related movement disorders. This doesn't mean every thyroid patient will develop Parkinson's. But it does mean that millions of people with thyroid disease may be experiencing symptoms that overlap with, mimic, or even contribute to parkinsonian conditions — and too often, no one is putting the pieces together.
This article is your guide to understanding that connection, recognizing the symptoms, navigating diagnosis, and taking an active role in your own neurological health.
Before we explore the thyroid connection, it's important to understand what we're talking about when we say "Parkinson's."
Parkinson's disease is a progressive neurodegenerative disorder caused primarily by the loss of dopamine-producing neurons in a region of the brain called the substantia nigra. Dopamine is a neurotransmitter that coordinates smooth, controlled movement. When those neurons die, movement becomes slow, rigid, and difficult to initiate.
The classic motor symptoms of Parkinson's disease are:
- Tremor — usually a "resting tremor," meaning the shaking is most noticeable when the limb is at rest and tends to diminish with movement
- Bradykinesia — slowed movement; tasks that once felt automatic (buttoning a shirt, writing, walking) become effortful and deliberate
- Rigidity — stiffness and resistance in the muscles and joints, often described as a "lead pipe" or "cogwheel" sensation
- Postural instability — impaired balance and difficulty with posture, often appearing later in the disease
- Hypomimia — a reduced or "masked" facial expression, where the face loses its natural animation
- Micrographia — handwriting that becomes progressively smaller and cramped
But Parkinson's is far more than a movement disorder. Non-motor symptoms are often equally — or more — debilitating, and include depression, anxiety, cognitive changes and dementia, sleep disturbances (particularly REM sleep behavior disorder), loss of smell (anosmia), constipation, and autonomic dysfunction (blood pressure drops, bladder issues, sweating abnormalities).
<h2 id="parkinsonian">What are parkinsonian syndromes?</h2>
Parkinsonian syndromes (also called atypical parkinsonism) are a family of conditions that share features with Parkinson's disease but have different causes, progression patterns, and responses to treatment. These include:
- Multiple system atrophy (MSA) — involves autonomic failure, cerebellar symptoms, and poor response to levodopa
- Progressive supranuclear palsy (PSP) — characterized by falls, vertical gaze palsy, and frontal-lobe-type dementia
- Corticobasal degeneration (CBD) — features asymmetric limb rigidity, apraxia, and alien limb phenomenon
- Lewy body dementia (LBD) — hallucinations, fluctuating cognition, and parkinsonism occurring alongside dementia
- Vascular parkinsonism — caused by small strokes affecting the basal ganglia and white matter
Parkinsonian mimics are conditions that can look exactly like Parkinson's but are caused by something else entirely — and are often reversible when the underlying cause is treated. This is where thyroid disease enters the picture in a profound way.
The numbers are striking. A 2022 systematic review analyzed data from nine studies and found that both hypothyroidism and hyperthyroidism are associated with meaningfully elevated risk of developing Parkinson's disease. The analysis found that patients with either form of thyroid dysfunction carried approximately 1.6 times the risk of developing Parkinson’s compared to individuals with normal thyroid function — a finding that reached statistical significance across multiple study designs.
A large landmark Swedish study followed more than 34,000 patients hospitalized with Hashimoto's disease or hypothyroidism and found a nearly 1.93-fold increased risk of developing Parkinson's disease. That means people with Hashimoto's or hypothyroidism were almost twice as likely to later develop Parkinson’s than the general population.
An even broader Swedish study of more than 300,000 subjects found that patients with autoimmune diseases — including Hashimoto's thyroiditis and hypothyroidism — had an additional 33% increased risk of Parkinson's disease compared to those without autoimmune conditions.
These are not small, clinically irrelevant numbers. They suggest a real biological relationship that the medical community is only beginning to take seriously.
<h2 id="thyroid-brain">Thyroid hormones and your brain</h2>
To understand why thyroid disease and Parkinson's are connected, you need to understand the role thyroid hormones play in the brain — particularly the role of T3 (triiodothyronine), the active form of thyroid hormone.
T3 and dopamine: An intimate relationship
Research published in 2019 made a remarkable discovery: T3 and T4 were identified as key factors for the induction of dopamine neurons. When scientists exposed neural precursor cells to thyroid hormones, the cells differentiated into dopamine-producing neurons. Remove the thyroid hormones, and dopamine neuron development was impaired. This finding established that thyroid hormones aren't just metabolic regulators — they are essential architects of the dopaminergic system that Parkinson's disease destroys.
The dopamine-thyroid axis: a two-way street
The relationship runs in both directions. As documented in a 2020 journal article, the dopaminergic system is deeply interconnected with the hypothalamic-pituitary-thyroid (HPT) axis. Dopamine upregulates thyrotropin-releasing hormone (TRH) while simultaneously downregulating TSH. Conversely, TRH stimulates dopamine release. This creates a feedback loop in which thyroid dysfunction and dopamine deficiency can amplify each other.
When dopamine-producing neurons die in Parkinson's disease, this disrupts thyroid axis regulation. And when thyroid hormones fall, dopamine neuron health is compromised. It's a vicious cycle.
Reverse T3: A smoking gun in Parkinson's?
One particularly telling piece of evidence involves reverse T3 — the biologically inactive form of T3 that is produced when the body converts T4 through an alternate pathway. Critically, T3 and reverse T3 are competitive: when reverse T3 goes up, active T3 goes down.
A study published in 2022 found that patients with Parkinson's disease had significantly elevated levels of reverse T3 compared to controls. Since elevated reverse T3 is a hallmark of functional hypothyroidism, the researchers interpreted this as evidence that low functional T3 — the active hormone the brain needs — is closely linked to Parkinson's disease pathology. Even when standard lab tests show "normal" thyroid function, elevated reverse T3 may indicate that the brain is not receiving enough active thyroid hormone.
This has enormous implications for thyroid patients. Many people with Hashimoto's have elevated reverse T3 even when their TSH appears normal — a pattern called T3/reverse T3 imbalance or functional hypothyroidism. These patients often report ongoing symptoms despite being told their labs are "fine."
Shared genes
The link between Hashimoto's and Parkinson's isn't only hormonal — it's also genetic. The LRRK2 gene, one of the most well-known genetic risk factors for Parkinson's disease, is highly expressed in immune cells and has been shown to influence both Parkinson’s and thyroid disease through immune mechanisms. Research has found that two-thirds of patients with LRRK2-associated Parkinson's developed autoimmune diseases including Hashimoto's thyroiditis. This genetic overlap suggests these diseases may share common immune pathways, not just coincidental comorbidities.

One of the most important and underdiagnosed conditions in this space is Hashimoto's encephalopathy (HE), also called Steroid-Responsive Encephalopathy Associated with Autoimmune Thyroiditis (SREAT). It is, in a very real sense, the brain expression of Hashimoto's autoimmunity.
First described in 1966, HE/SREAT is a neurological condition characterized by disease or dysfunction of the brain that alters its structure or function (encephalopathy), thyroid autoimmunity (elevated anti-TPO or anti-thyroglobulin antibodies), and — critically — a striking response to corticosteroid treatment. It affects an estimated 2.1 per 100,000 people, predominantly women, and is believed to be significantly underdiagnosed.
Here is the most important thing to understand about HE/SREAT: you can have it even if your thyroid function tests are normal. Up to 30% of patients with confirmed HE/SREAT are euthyroid (normal thyroid function) at the time of presentation. The presence of thyroid antibodies — particularly anti-TPO antibodies — is the diagnostic clue, not the thyroid hormone levels themselves. This means patients with Hashimoto's who are being told their T4 and TSH are "normal" may still be developing HE/SREAT.
HE/SREAT presents with an extraordinary range of neurological and psychiatric symptoms, many of which look startlingly similar to Parkinson's disease and other movement disorders. These include:
- Tremor — one of the most common motor manifestations
- Myoclonus — sudden, brief muscle jerks (present in 42–65% of patients in larger case series)
- Ataxia — impaired coordination and gait (present in 33–65% of cases)
- Cognitive impairment — memory problems, confusion, slowed thinking
- Altered consciousness — ranging from confusion to coma
- Psychiatric symptoms — hallucinations, paranoia, psychosis, personality changes
- Seizures — including generalized tonic-clonic and partial seizures
- Speech problems — transient aphasia or dysarthria
- Sleep disturbances and depression
- Movement disorders broadly — including gait abnormalities that can resemble parkinsonism
Crucially, HE/SREAT can present in a relapsing-remitting pattern, meaning symptoms come and go, which can lead to years of misdiagnosis. The condition has been mistaken for multiple sclerosis, Creutzfeldt-Jakob disease, Lewy body dementia, and — most relevantly for this discussion — Parkinson's disease and parkinsonian syndromes.
You can learn more about the diagnosis and treatment of Hashimoto’s encephalopathy in an in-depth article from Paloma.
Separate from HE/SREAT, hypothyroidism itself can directly produce a full parkinsonian syndrome — and the most important feature of hypothyroid-induced parkinsonism is that it is potentially reversible with appropriate thyroid hormone treatment.
Hypothyroidism may be associated with both hypokinetic disorders (slowed movement) and hyperkinetic disorders (excessive movement), and the coexistence of hypothyroidism and Parkinson's disease can be a major source of diagnostic delay and confusion.
The overlapping symptom problem
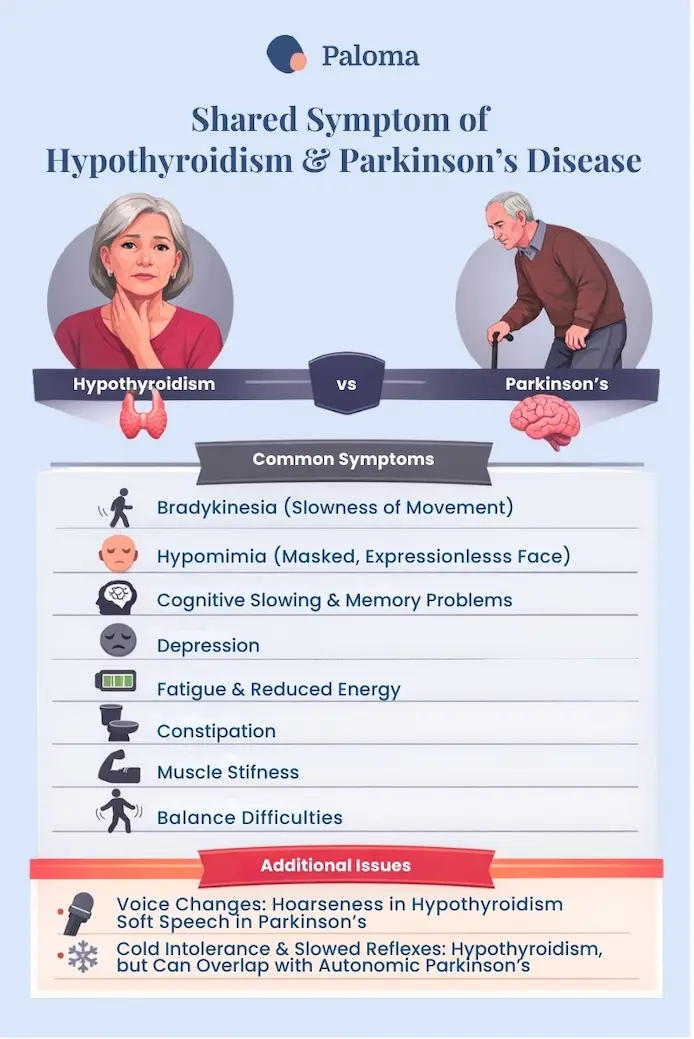
Consider the symptoms that hypothyroidism and Parkinson's disease share:
- Bradykinesia (slowness of movement) — present in both
- Hypomimia (masked, expressionless face) — present in both
- Cognitive slowing and memory problems — present in both
- Depression — present in both
- Fatigue and reduced energy — present in both
- Constipation — present in both
- Muscle stiffness — present in both
- Balance difficulties — present in both
- Voice changes — hoarseness in hypothyroidism; soft speech in Parkinson’s disease
- Cold intolerance and slowed reflexes — hypothyroidism, but can overlap with autonomic Parkinson’s disease
This overlap means that a patient with undiagnosed or inadequately treated hypothyroidism may receive a Parkinson's diagnosis in error. Conversely, developing hypothyroidism in the course of Parkinson's disease can go undetected for years, because the symptoms of hypothyroidism are attributed to worsening Parkinson's.
One documented case from the literature describes a woman who had Parkinson's disease for 17 years before developing unexplained "on-off fluctuations" that no longer responded to her usual medications. The real culprit was undiagnosed hypothyroidism — and when that was treated with thyroid hormone replacement, her Parkinson's fluctuations were controlled. This case powerfully illustrates how thyroid hormone status influences dopaminergic metabolism in real patients.
Another case report described a patient with Parkinson’s disease who accidentally stopped taking his levothyroxine for two months after a thyroidectomy. His parkinsonism, psychosis, myoclonus, and encephalopathy all dramatically worsened. After levothyroxine was restarted, his condition stabilized within 10 days — demonstrating that hypothyroidism can cause reversible myoclonus and encephalopathy on top of existing Parkinson’s disease.
There is currently no single blood test or scan that definitively confirms Parkinson's disease. Diagnosis is primarily clinical — based on the neurologist's observation of symptoms and the patient's history. The cardinal features that must be present are bradykinesia (slowness) combined with either rigidity, resting tremor, or postural instability. The diagnosis is supported by a positive response to levodopa therapy.
Several tools help confirm or differentiate Parkinson’s disease:
DaTscan (Dopamine Transporter Scan)
This nuclear imaging test uses a radioactive tracer called Ioflupane I 123 that binds to dopamine transporters in the brain. In true Parkinson's disease, the scan shows a characteristic reduction in dopamine transporter activity— a "comma" shape reduces to a "period." The DaTscan is useful for distinguishing Parkinson’s from essential tremor (which shows a normal scan), but it cannot distinguish between Parkinson's disease and the atypical parkinsonian syndromes. Critically for thyroid patients, a normal DaTscan in someone with parkinsonian symptoms should trigger a thorough search for secondary causes — including thyroid dysfunction.
Brain MRI
An MRI of the brain is used primarily to rule out structural causes of parkinsonism, such as vascular disease or tumors. Certain patterns on MRI can suggest atypical parkinsonian syndromes.
Neurological examination
Neurological assessment includes evaluation of gait, facial expression, handwriting, finger-tapping speed, rigidity, and balance.
A levodopa challenge iss an important part of the Parksinson’s disease diagnostic process. Levodopa (often combined with carbidopa as Sinemet or benserazide as Madopar) remains the most effective medication for Parkinson’s disease. The drug crosses the blood–brain barrier and converts into dopamine—the neurotransmitter depleted as Parkinson’s progressively destroys dopamine-producing neurons in the brain. Restoring dopamine improves hallmark motor symptoms such as slowness, stiffness, and difficulty initiating movement.
Because levodopa directly targets dopamine deficiency, a strong improvement after taking the drug supports a diagnosis of Parkinson’s disease. Little or no improvement suggests another cause for the movement disorder.
This is the basis of the levodopa challenge trial, in which motor function is scored before and after dosing using standardized evaluation tools.
A clear and sustained improvement on levodopa strongly supports Parkinson’s disease.
What a failed levodopa trial can mean
If symptoms do not improve, neurologists typically consider three broad explanations.
Atypical neurodegenerative parkinsonism
Conditions such as progressive supranuclear palsy (PSP), multiple system atrophy (MSA), corticobasal degeneration (CBD), and Lewy body dementia share parkinsonian features but involve broader brain degeneration.
These atypical disorders damage not only dopamine-producing neurons but also dopamine receptors in the striatum. Without functioning receptors, levodopa has little effect.
Clinical red flags include:
- Rapid disease progression
- Early falls or gait instability
- Prominent autonomic dysfunction
- Minimal tremor
- Poor levodopa response
Secondary parkinsonism
Symptoms may also arise from non-degenerative causes, including:
- Medication effects (antipsychotics, antiemetics, calcium channel blockers)
- Vascular injury from small strokes
- Normal pressure hydrocephalus
- Toxin exposure
In these cases dopamine production may be normal, but movement circuits are disrupted elsewhere. Clinical guidelines often define levodopa failure as less than 25% improvement despite adequate dosing.
Thyroid-related parkinsonism — a reversible cause
For people with Hashimoto’s or hypothyroidism, a failed levodopa trial may instead point to thyroid dysfunction.
Movement symptoms caused by thyroid hormone deficiency do not respond to levodopa, because the underlying issue is not dopamine depletion. Instead, low thyroid hormone disrupts metabolic and neurological processes throughout the brain and nervous system.
In this situation, the correct treatment is thyroid hormone replacement—not dopamine therapy.
The levodopa–thyroid connection
Because levodopa converts to dopamine, it can suppress TSH secretion. Patients taking levodopa may therefore show artificially low or normal TSH levels, even when thyroid hormone activity is inadequate.
Studies have documented altered thyroid feedback responses in patients on levodopa therapy.
For this reason, thyroid evaluation should include:
- Free T4
- Free T3
- Reverse T3
—not just TSH.
It’s also important to note levodopa can temporarily affect thyroid testing. Dopamine suppresses TSH secretion, so levodopa may lower TSH for several hours after dosing, potentially confusing lab interpretation.
For thyroid patients undergoing a levodopa challenge, thyroid labs should ideally be drawn before the test, not afterward.
Next steps after a failed levodopa trial
Before concluding the trial truly failed, clinicians should confirm that testing conditions were appropriate. False negatives can occur if the dose was too low, the medication was taken with protein (which interferes with absorption), the trial was too short, or thyroid dysfunction affected the dopaminergic response. Even some patients with confirmed Parkinson’s initially show little improvement.
A comprehensive thyroid evaluation is essential in patients with suspected thyroid disease. Testing should include TSH, free T4, free T3, reverse T3, and thyroid antibodies.
If hypothyroidism is identified, treatment should be optimized before drawing neurological conclusions. Hypothyroid-related parkinsonism can improve significantly once thyroid hormone levels normalize. Case reports describe Parkinson-like symptoms resolving after treatment of severe hypothyroidism.
Persistent neurological symptoms may require evaluation for HE/SREAT.
When diagnosis remains uncertain, a DaTscan can evaluate dopamine transporter activity in the brain. A normal scan largely rules out Parkinson’s disease and points toward secondary or reversible causes—including thyroid dysfunction.
Atypical parkinsonian syndromes are often diagnosed based on specific clinical patterns:
- PSP: Early falls, vertical gaze palsy (inability to look up or down), frontal cognitive changes, and poor levodopa response
- MSA: Autonomic failure (orthostatic hypotension, bladder problems), cerebellar features, and poor levodopa response
- CBD: Asymmetric limb rigidity with apraxia, alien limb phenomenon
- Lewy Body Dementia: Dementia preceding or within 1 year of parkinsonism, visual hallucinations, fluctuating cognition
For these conditions, neuroimaging with MRI, functional imaging (PET, DaTscan), and detailed neuropsychological testing are all part of the diagnostic workup.
When thyroid disease may be involved in neurological symptoms, the following testing is essential:
Comprehensive thyroid panel
This should go beyond a simple TSH test. An adequate panel for someone with neurological symptoms includes TSH, free T4, free T3, reverse T3, anti-TPO antibodies, and anti-thyroglobulin antibodies. The free T3 level and the T3/reverse T3 ratio are particularly important because patients can have "normal" TSH and T4 while still being functionally hypothyroid — meaning the brain isn't getting enough active thyroid hormone.
Anti-TPO and anti-Tg antibodies
These thyroid antibodies are the markers for Hashimoto's thyroiditis and are essential for diagnosing HE/SREAT. The key diagnostic finding for HE/SREAT is the presence of these antibodies in the context of encephalopathy, not their specific level.
CSF (cerebrospinal fluid) analysis
In suspected HE/SREAT, a lumbar puncture may reveal elevated protein and mild inflammatory changes — a non-specific finding but supportive of the diagnosis. Importantly, CSF analysis in HE/SREAT does NOT typically show the oligoclonal bands seen in MS, helping differentiate the two.
EEG (electroencephalogram)
Almost universally abnormal in HE/SREAT (in 98% of cases), typically showing diffuse slowing — a finding that can help distinguish HE/SREAT from Parkinson's disease, which does not typically alter the EEG.
Diagnosis of HE/SREAT
Requires encephalopathy with cognitive impairment, the presence of antithyroid antibodies, no evidence of infectious or structural brain disease, and ideally a positive response to steroids.
Perhaps the most actionable area in the thyroid-brain connection is the role of free T3 and the growing evidence that many thyroid patients are living with insufficiently treated thyroid disease because their T3 levels are never properly evaluated.
Why standard T4 treatment may leave the brain underpowered
The standard treatment for hypothyroidism in most countries is levothyroxine — the synthetic version of T4, the storage form of thyroid hormone. The body is supposed to convert T4 to the active T3 hormone through enzymes called deiodinases. However, this conversion is impaired in many people, particularly those with Hashimoto's disease, chronic inflammation, high stress, certain nutrient deficiencies, and genetic variants in deiodinase enzymes.
When T4-to-T3 conversion is impaired:
- Free T3 levels remain low despite "normal" TSH and T4
- Reverse T3 may be elevated, further blocking T3 action at the cellular level
- The brain — which requires substantial local T3 for dopamine neuron health — may be chronically understimulated
The significant increase in reverse T3 observed in Parkinson's disease patients is evidence that hypothyroidism is closely related to the occurrence of Parkinson’s disease. This pattern — elevated reverse T3 coexisting with suboptimal free T3 — is something many integrative and functional medicine practitioners see routinely in Hashimoto's patients, and it may have neurological consequences that standard thyroid care ignores.
The case for monitoring free T3
Research published in the International Journal of Neuroscience found that thyroid hormone levels and structural parameters of thyroid homeostasis were correlated with motor subtype and disease severity in patients with Parkinson's disease — even in patients who appeared euthyroid by standard testing. This suggests that the nuances of thyroid hormone metabolism have real-world consequences for movement and brain function.
For thyroid patients who have neurological symptoms, experts increasingly recommend:
- Testing free T3 (not just TSH and free T4) at every evaluation
- Testing reverse T3 if free T3 appears low or symptoms persist
- Calculating the T3/reverse T3 ratio — a value below approximately 20 (when both are measured in the same units) may indicate functional hypothyroidism
- Testing anti-TPO and anti-thyroglobulin antibodies if not already done
T3 combination therapy: An evolving conversation
Some endocrinologists and thyroid specialists now offer combination therapy with both levothyroxine (T4) and liothyronine (T3, synthetic T3) for patients who continue to have symptoms despite optimal T4 therapy. The evidence base for this approach is growing, particularly for patients with polymorphisms in the DIO2 gene who cannot efficiently convert T4 to T3
For patients with neurological symptoms resembling parkinsonism, ensuring adequate T3 levels — whether through improved conversion or direct T3 supplementation — may be particularly important, given the evidence that T3 directly supports dopamine neuron health and survival.
<div id="schedule_snippet_2" class="max-width _700 doctor-ads"><h1 class="heading-2 hero v2 chechkout-right-copy">Dealing with Hypothyroidism? Video chat with a thyroid doctor</h1><h5 class="heading-3 centered left leftyer">Get answers and treatments in minutes without leaving home - anytime. Consult with a U.S. board certified doctor who only treats hypothyroidism via high-quality video. Insurance accepted.</h5><a href="https://app.palomahealth.com/book-appointment/" target="_blank" class="button spacing orange w-button">Schedule</a></div>
If you have Hashimoto's or hypothyroidism and are experiencing symptoms that resemble parkinsonism:
Step 1: Don't dismiss the symptoms.
Tremor, slowness, stiffness, masked expression, balance problems, and cognitive fog in a thyroid patient should never be attributed solely to thyroid disease without investigation — but they should also never be attributed to Parkinson's disease without first optimizing thyroid treatment.
Step 2: Get a complete thyroid panel.
Request TSH, free T4, free T3, reverse T3, anti-TPO antibodies, and anti-thyroglobulin antibodies. If your provider refuses to test free T3 or reverse T3, consider seeking care from Paloma Health’s expert providers, an integrative medicine physician, or functional medicine doctor with thyroid expertise.
Step 3: Optimize your thyroid treatment.
If free T3 is low or reverse T3 is elevated, work with your provider to optimize your thyroid replacement — whether through adjusting levothyroxine dose, addressing conversion issues (nutrient deficiencies, chronic inflammation), or potentially transitioning to combination T4/T3 therapy or a desiccated thyroid extract.
Step 4: Give optimization time.
Hypothyroid-induced parkinsonism and neurological symptoms from low T3 can take weeks to months to reverse after thyroid hormone levels are optimized. This is not a quick fix, but resolution of reversible neurological symptoms has been documented in the literature.
Step 5: See a neurologist.
Any thyroid patient with persistent tremor, gait changes, balance problems, cognitive decline, or symptoms that don't resolve with thyroid optimization should see a neurologist for formal evaluation. A neurologist can:
- Conduct a complete movement disorder exam
- Order a DaTscan if needed
- Rule out Parkinson's disease or atypical parkinsonian syndromes
- Consider HE/SREAT in the differential diagnosis
Step 6: If HE/SREAT is suspected — advocate for diagnosis and treatment!
HE/SREAT is chronically underdiagnosed. If you have Hashimoto's, elevated anti-TPO antibodies, and neurological symptoms that include cognitive changes, tremor, myoclonus, seizures, or movement difficulties — especially if those symptoms fluctuate — ask your neurologist to consider HE/SREAT. Key diagnostic steps include checking for elevated anti-TPO in serum and possibly CSF, an EEG, MRI brain, and a trial of corticosteroids.
The cornerstone of treatment for HE/SREAT is corticosteroids, (typically prednisone 50–150 mg/day or high-dose IV methylprednisolone) and the response can be dramatic and life-changing. Many patients experience remarkable neurological improvement within weeks. For patients who relapse or do not fully respond to steroids, second-line options include azathioprine, mycophenolate mofetil, or intravenous immunoglobulin (IVIG).
Importantly, HE/SREAT does not necessarily require hypothyroidism to be treated — the autoimmune mechanism affecting the brain may operate independently of thyroid hormone levels. Thyroid hormone replacement should be optimized in patients who are hypothyroid, but steroid treatment targets the immune process, not the thyroid hormone deficiency.
For patients already diagnosed with Parkinson’s disease
If you have Parkinson's and also have Hashimoto's or hypothyroidism, your case warrants special attention:
- Thyroid function should be assessed regularly, not just at diagnosis
- If your Parkinson's symptoms are worsening or not responding to medications in the expected way, request a full thyroid panel — including free T3 and reverse T3
- Treating newly developed or worsening hypothyroidism in a Parkinson’s disease patient can meaningfully improve symptom control, as multiple case reports have demonstrated
- If you are taking levodopa, be aware that dopaminergic medications can affect TSH levels and complicate interpretation of standard thyroid labs
Ongoing: Incorporate physical activity

One of the most important first steps you can take after a diagnosis of Parkinson's disease or parkinsonian symptoms is to incorporate exercise into your overall treatment plan.
Nina Mosier, MD, Co-Founder and Executive Director of Power for Parkinson's explains:
"Exercise has been proven in study after study to reduce the side effects of Parkinson's. So, most neurologists will recommend an exercise regimen during the initial Parkinson's diagnosis visit, alongside medication. Exercise is one of the most powerful tools we have to address Parkinson’s symptoms, including mobility, balance, cognition, mood, and confidence.
Ongoing: Get support
Power for Parkinson’s cofounder Dr. Mosier also says that patients should not underestimate the value of support and social connection. Says Dr. Mosier: “Isolation can make Parkinson’s feel harder. Community, care partners, and ongoing encouragement help people stay motivated, active, and living as fully as possible.”
The emerging science points to a fundamental insight: autoimmune diseases and neurodegeneration may share common roots. The same immune dysregulation that leads the body to attack its own thyroid appears, in some individuals, to also prime the nervous system for inflammatory and degenerative processes.
Neuroinflammation, once thought to be a secondary feature of Parkinson’s disease, is now recognized as a central driver — and this same inflammatory situation characterizes Hashimoto's disease.
For researchers, there’s an interesting question: could optimizing thyroid function — particularly ensuring adequate free T3 — serve as a modifiable protective factor against Parkinson's disease? As a 2022 study concluded, thyroid hormone signaling plays an essential role in the development of Parkinson’s disease and overt thyroid dysfunction could be a modifiable risk factor for Parkinson’s disease. This is, potentially, one of the most important findings in recent neurology research for the thyroid community.
If you have Hashimoto's, hypothyroidism, or any autoimmune thyroid disease and are concerned about neurological symptoms, ask these questions during your next appointment:
- "Can we check my free T3 and reverse T3 levels, in addition to TSH and free T4?"
- "Are my anti-TPO antibodies elevated? Have they been checked recently?"
- "I've been experiencing [tremor / slowness / balance issues / cognitive fog / muscle stiffness]. Could this be related to my thyroid, or do I need a neurological evaluation?"
- "Is my T3/reverse T3 ratio in a healthy range?"
- "Should I be referred to a neurologist or movement disorder specialist?"
- "Could I have HE/ SREAT? What would be the diagnostic workup?"
The connection between thyroid disease and Parkinson's/parkinsonian syndromes is real, it is increasingly supported by science, and it is clinically important — but it is not a sentence. The evidence does not mean that Hashimoto's disease causes Parkinson's in all or even most patients. It means there is a biologically meaningful relationship that deserves attention, monitoring, and research.
The most hopeful implication of all this research is the concept of reversibility. Hypothyroid-induced parkinsonism can resolve. HE/SREAT responds dramatically to steroids. Suboptimal T3 levels can be corrected. Unlike true Parkinson's disease, which is progressive and incurable, many of the neurological complications arising from thyroid dysfunction are treatable — if they are recognized in time.
The lesson for every thyroid patient is this: know your full thyroid panel, monitor your neurological health, advocate for comprehensive care, keep moving, and don't let symptoms that cross the thyroid-brain boundary go unexplained. The science is showing us that these two systems are profoundly connected — and understanding that connection may protect not just your thyroid, but your brain.
If you need thyroid care that includes full thyroid panels, and optimal hypothyroidism treatment, learn more about becoming a Paloma Health patient.
What is the connection between thyroid disease and Parkinson’s disease?
Research suggests thyroid dysfunction—especially hypothyroidism and autoimmune thyroid disease like Hashimoto’s—may increase the risk of developing Parkinson’s disease. Scientists believe the link involves thyroid hormones’ role in maintaining dopamine-producing brain cells and regulating neurological function.
Can hypothyroidism cause symptoms that look like Parkinson’s?
Yes. Hypothyroidism can cause tremor, slow movement, muscle stiffness, balance problems, fatigue, and cognitive slowing. Because these symptoms overlap with Parkinson’s disease, thyroid problems can sometimes be mistaken for a movement disorder if thyroid function isn’t thoroughly evaluated.
What are the most common symptoms of Parkinson’s disease?
The classic symptoms include tremor, slowed movement (called bradykinesia), muscle rigidity, and balance problems. Many people also experience non-motor symptoms such as sleep disturbances, depression, constipation, loss of smell, and cognitive changes.
Why are thyroid hormones important for brain health?
Thyroid hormones play a key role in brain metabolism, nerve signaling, and the development of dopamine neurons. These neurons help control smooth movement and coordination, which is why disruptions in thyroid hormone levels can affect neurological function.
What is reverse T3 and why does it matter?
Reverse T3 is an inactive form of thyroid hormone that can block the action of active T3 in cells. High reverse T3 levels may indicate that the body isn’t effectively using thyroid hormone, which could contribute to symptoms like fatigue, brain fog, and potentially neurological issues.
What is Hashimoto’s encephalopathy?
Hashimoto’s encephalopathy is a rare autoimmune condition associated with Hashimoto’s disease that affects the brain. It can cause tremor, confusion, seizures, movement problems, and psychiatric symptoms—but it often improves dramatically with steroid treatment.
Can Parkinson-like symptoms from thyroid disease be reversible?
In some cases, yes. When neurological symptoms are caused by hypothyroidism or thyroid hormone imbalance, they may improve or resolve once thyroid hormone levels are properly treated and stabilized.
How is Parkinson’s disease diagnosed?
There is no single test for Parkinson’s disease. Doctors typically diagnose it based on symptoms, neurological examination, and response to medications like levodopa. Imaging tests such as a DaTscan may help support the diagnosis or rule out other causes.
Why might a Parkinson’s medication not work for some people?
If levodopa or other Parkinson’s medications don’t improve symptoms, it may suggest the symptoms are caused by something other than dopamine loss. Possible explanations include atypical parkinsonian disorders, medication side effects, vascular damage, or thyroid-related conditions.
What should someone with thyroid disease do if they develop neurological symptoms?
If you have Hashimoto’s or hypothyroidism and develop tremor, balance problems, stiffness, or cognitive changes, it’s important to discuss these symptoms with your doctor. A comprehensive thyroid panel and evaluation by a neurologist can help determine whether the symptoms are related to thyroid dysfunction, Parkinson’s disease, or another neurological condition.


.webp)








